Chapter 21
An overview of donor wellness and perspectives
Chapter highlights
Summary of the chapter:
- Donor wellness is critical for a sustainable blood system.
- Blood system characteristics vary between jurisdictions and knowledge of the local blood system is important to better understand nuances of donor and recipient safety.
- Understanding donor motivations and barriers helps improve recruitment and retention through the creation of safe, positive donation experiences.
- Blood donation health benefits are not supported by published scientific data for most donors; however, there are specific medical conditions (i.e., hemochromatosis) where whole blood (red cell) donation is part of chronic management.
- Adverse events from blood, platelet, and plasma donations are uncommon, and some may even be preventable. Hence, rapid identification to aid treatment and development of donor safety protocols are crucial to minimizing these adverse reactions.
- Testing and deferral policies protect donor health, help maintain blood product quality, and recipient safety.
Learning objectives
After reading this chapter you will be able to:
- Describe the importance of donor wellness in sustaining a safe and reliable blood system
- Outline Canada’s contributions to the First and Second World War and how it helped pave the way for the modern civilian blood system
- Explain global disparities in blood supply and the most common donor deferral reasons in high-, middle-, and low-income countries.
- Recognize the societal-level influences that can impact peoples’ motivation to donate blood and/or plasma.
- Identify common adverse events and their mitigation strategies for both whole blood and apheresis donations.
Test your knowledge at the end of this chapter with practice questions.
Introduction
Donors are critical to the existence of the blood system and their ongoing participation underpins a secure blood supply, saves lives and is vital to the functioning of the health system. To recruit and retain a strong donor base, blood operators’ donation processes must be safe, efficient and meaningful for donors.
More information on the organization of the Canadian blood system is available in Chapter 1. Canadian Blood Services’ mandate is provided on our website.
The aim of this chapter is to present a short historical context for blood donation and discuss aspects of donor wellness and safety. This chapter includes information about donor motivations and deterrents, donation-related health impacts, and donation-related adverse events and their management.
Donor wellness in wartime
Donors provide a selfless service, saving and improving the lives of many people. Without their generosity, the foundation of the current public blood system would not exist. Civilian blood donations in support of wartime efforts paved the way for our current blood system and the history of this generosity is summarized in this section. Dr. Jean Wang, a Canadian physician with an interest in the history of transfusion medicine, has kindly shared images of posters, postcards, and stamps from her personal collection.1
Wartime blood donor recruitment
A public blood system, although a fundamental part of patient care today, is a relatively recent development. In the early 1900s, shortly before World War I, blood was first stored outside the human body and transfused with a rudimentary understanding of blood typing and donor-recipient compatibility testing. This was made possible with the discovery of the anticoagulant properties of sodium citrate, which prevented the clotting of stored, donated blood, allowing it to be “banked” for future transfusion.1 During World War I, wounded soldiers with less severe injuries became some of the first blood donors; however, as this supply was insufficient to meet the wartime demand, civilian donations became necessary.
In 1936, the first transfusion service with a civilian donor base was established by Dr. Frederic Durán Jorda in Barcelona, in response to the need for lifesaving transfusions during the Spanish Civil War.2 Then in 1937, Canadian surgeon Dr. Norman Bethune began a similar blood donor service in Madrid and developed a specialized vehicle with a kerosene-run refrigerator to create the “Servicio Canadiense de Transfusion de Sangre” (Canadian Blood Transfusion Service), a mobile transfusion service.1, 3, 4 Within 5 months of the launch of this program, Dr. Bethune’s team supplied blood across the 1000 km front line, providing up to 100 transfusions a day.3
Despite these advances in transfusion medicine at the time, the problem of short whole blood shelf-life remained. Research into extending the shelf-life of products led to interesting discoveries by Dr. Charles R. Drew, an African American surgeon trained at McGill University. His research refined methods for collecting, processing, and storing plasma, and as medical director of the “Blood for Britain” project in 1940, he introduced refrigerated trucks to transport blood and serve as collection centres; these vehicles were referred to as “bloodmobiles.” 5, 6
To support the war efforts in World War II, Canadian physician Dr. Charles Best helped develop methods to produce, store, and ship freeze-dried serum in glass bottles.7 The dried serum could be rehydrated with sterile distilled water and rapidly transfused to patients in need. The serum was lightweight and had a longer shelf-life than whole blood, which made it an important resource for saving lives on the front lines. During World War II, Canada became the largest producer of freeze-dried serum with more than 1 million litres of blood donated through over 2.3 million donations by Canadians. A majority of these donations were made by women.
To recruit donors, many campaigns were launched with a variety of slogans and messages. Many of the messages were disseminated with the help of the Canadian postal service. Postcards with patriotic images were mailed to advise donors of mobile blood donor clinics (see Figure 1), and slogans promoting blood donation were added to machine cancels of stamps on letters (see Figure 2). The Red Cross also distributed leaflets promoting blood donation (Figure 3).1 The messaging focused on wording to emphasize that donors were saving lives and stories designed to boost civilian morale.1 Importantly, the messaging in these campaigns also focused on maintaining donor wellness and improving the quality of the donation collected. They often provided suggestions for healthy meals before and after a whole blood donation for replenishing iron. At the time, donations with a high-fat content interfered with the production of the freeze-dried serum. As a result, promotional materials encouraged fat-free meals for up to 6 hours before donation (see Figure 4).
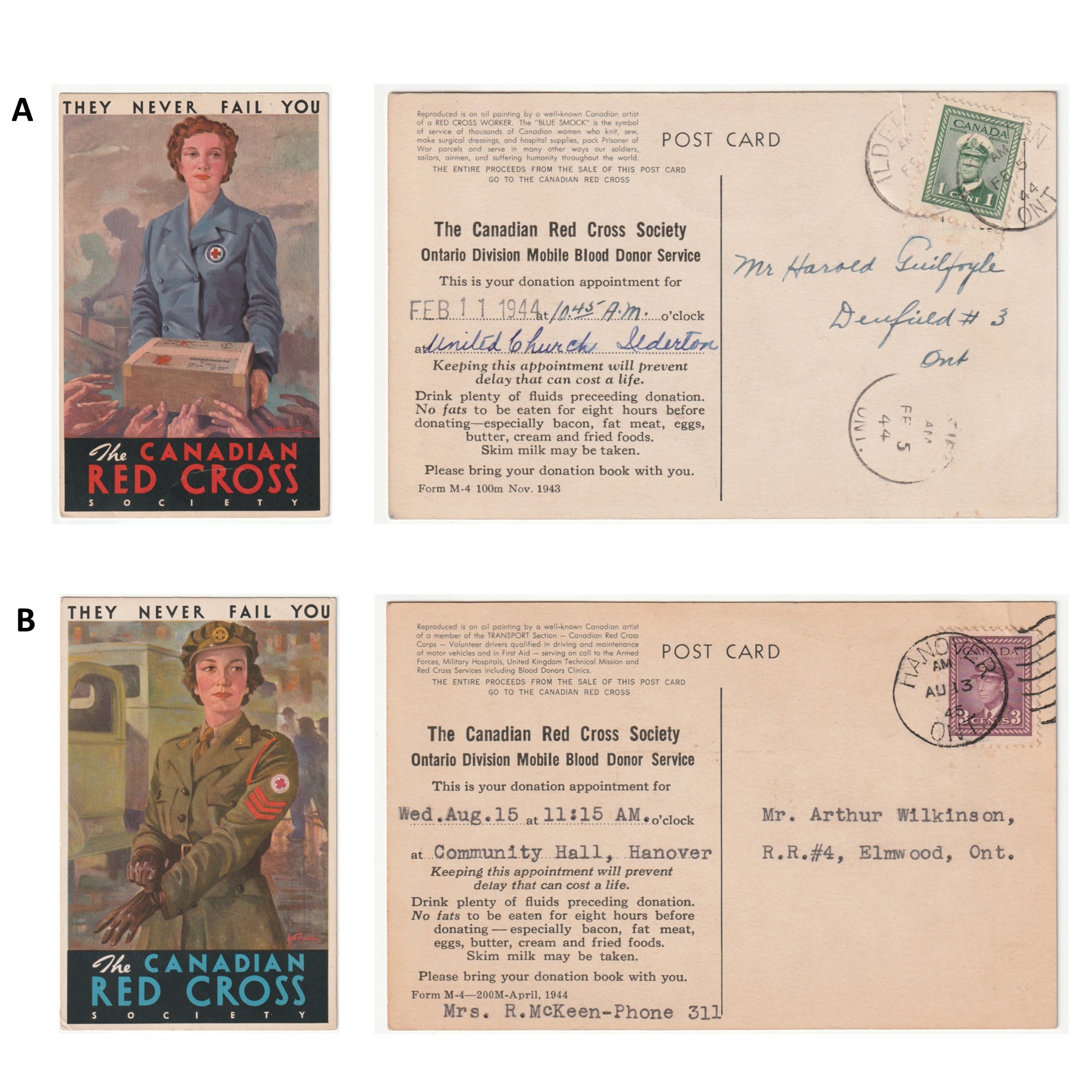
Figure 1. Postcards from the Canadian Red Cross Society bearing the motto “They Never Fail You” and depicting paintings of female World War II Red Cross Workers on the front and with mobile blood donor clinic appointment information printed on the backA. "Blue Smock” Red Cross worker, for a clinic in Ilderton, Ontario, B. Volunteer Driver, for a clinic in Elmwood, Ontario.
Images from the collection of Dr. Jean Wang, shared with her permission.

Figure 2. Machine cancels with slogans promoting blood donation used by the Canadian postal service during World War II. A. This slogan was used in Winnipeg from 1941 to 1942. B. This bilingual slogan was used in Ottawa from 1944 to 1945.
Images from the collection of Dr. Jean Wang, shared with her permission.
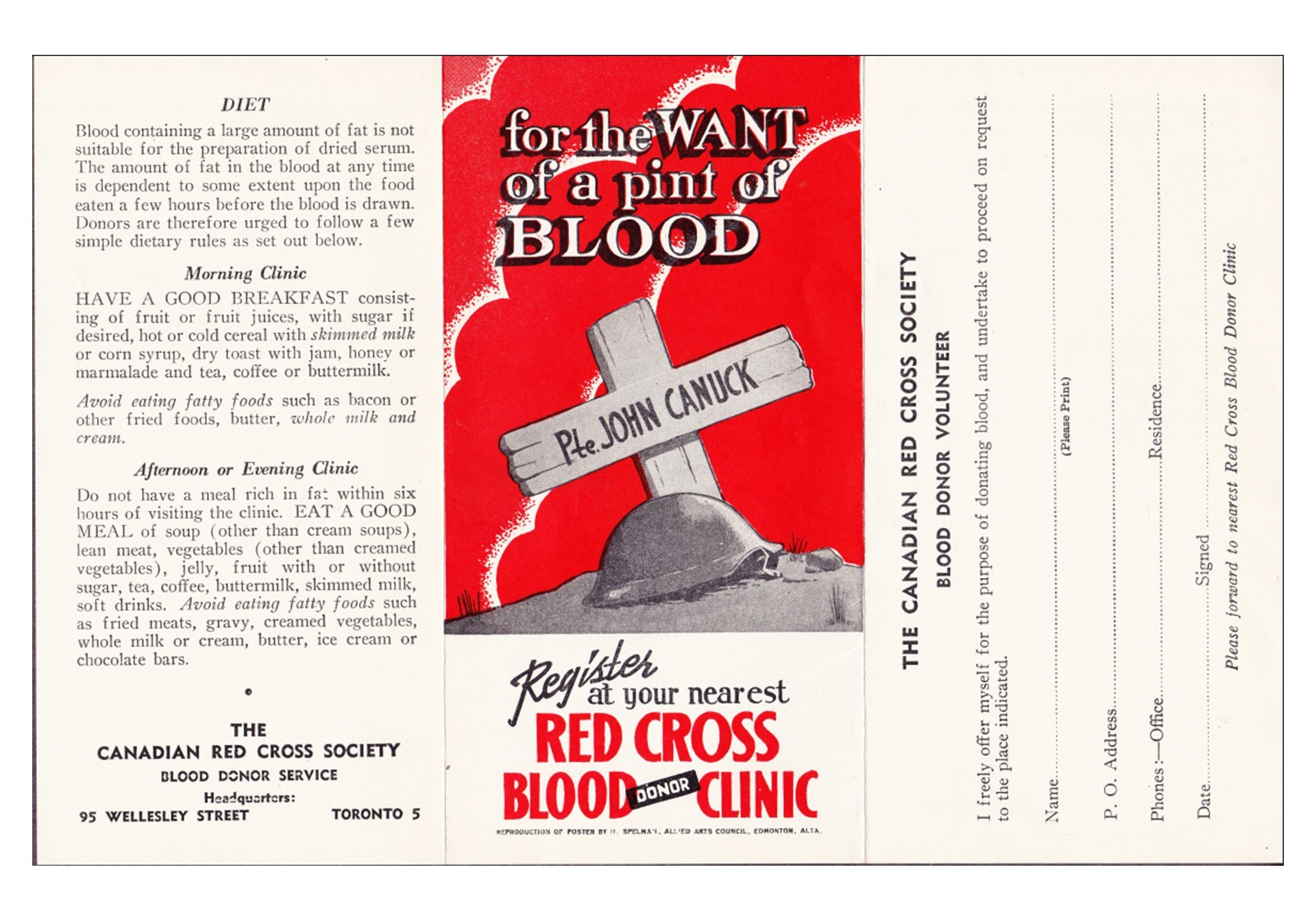
Figure 3. A 1944 World War II Canadian Red Cross leaflet providing information about blood donation and appealing for volunteer donors to support the production of dried serum. It depicts the tomb of Pte. John Canuck, a fictional Canadian war hero from cartoons of the time.
Used with permission from Dr. Jean Wang.
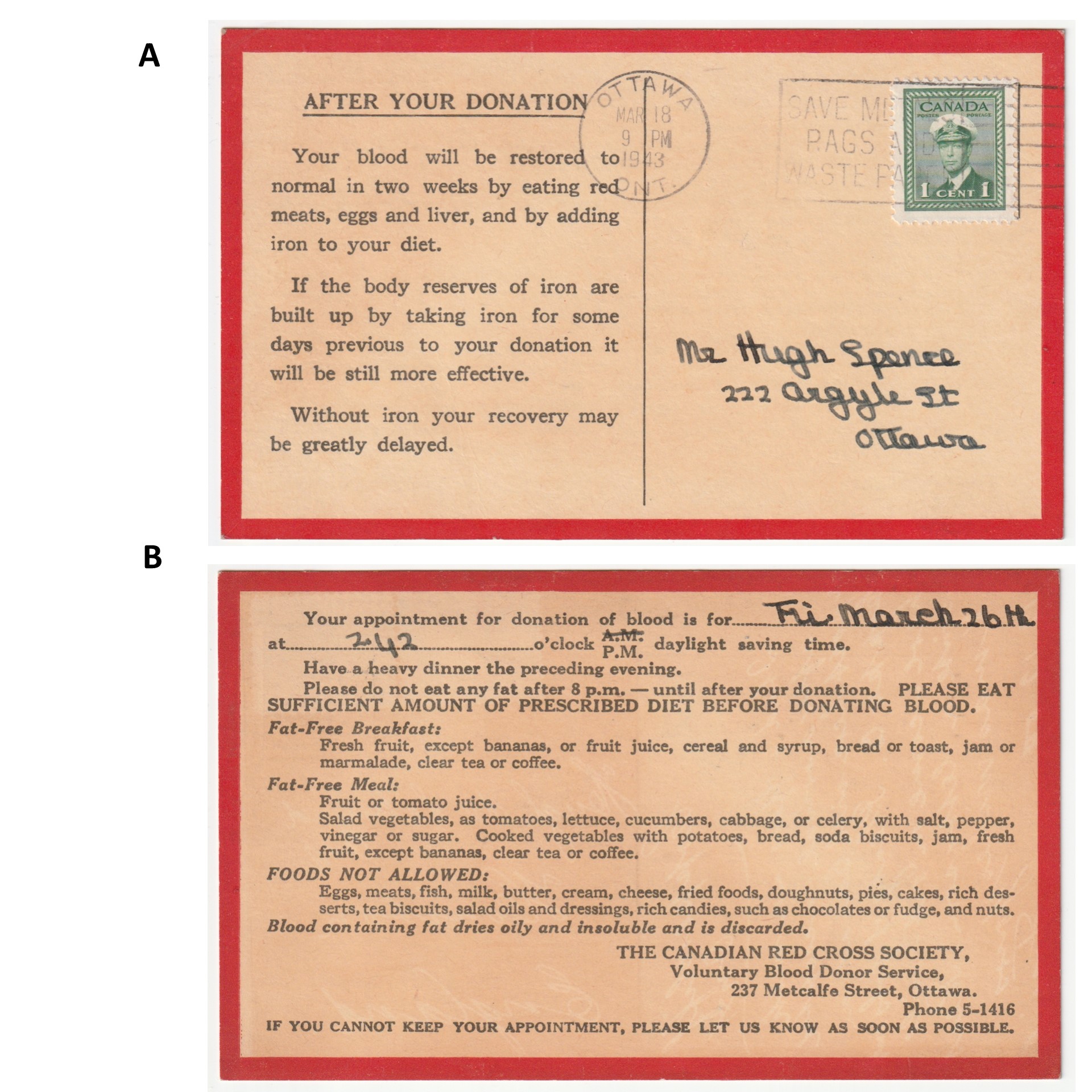
Figure 4. A 1943 postcard with dietary instructions for before and after your donation. A. Front of the postcard displaying a recommendation for food to eat after your blood donation in order to replenish iron, B. Back of the postcard with the appointment date and food to eat before your blood donation, emphasizing low fat to assist with the freeze-dried serum campaign.
Images from the collection of Dr. Jean Wang, shared with her permission.
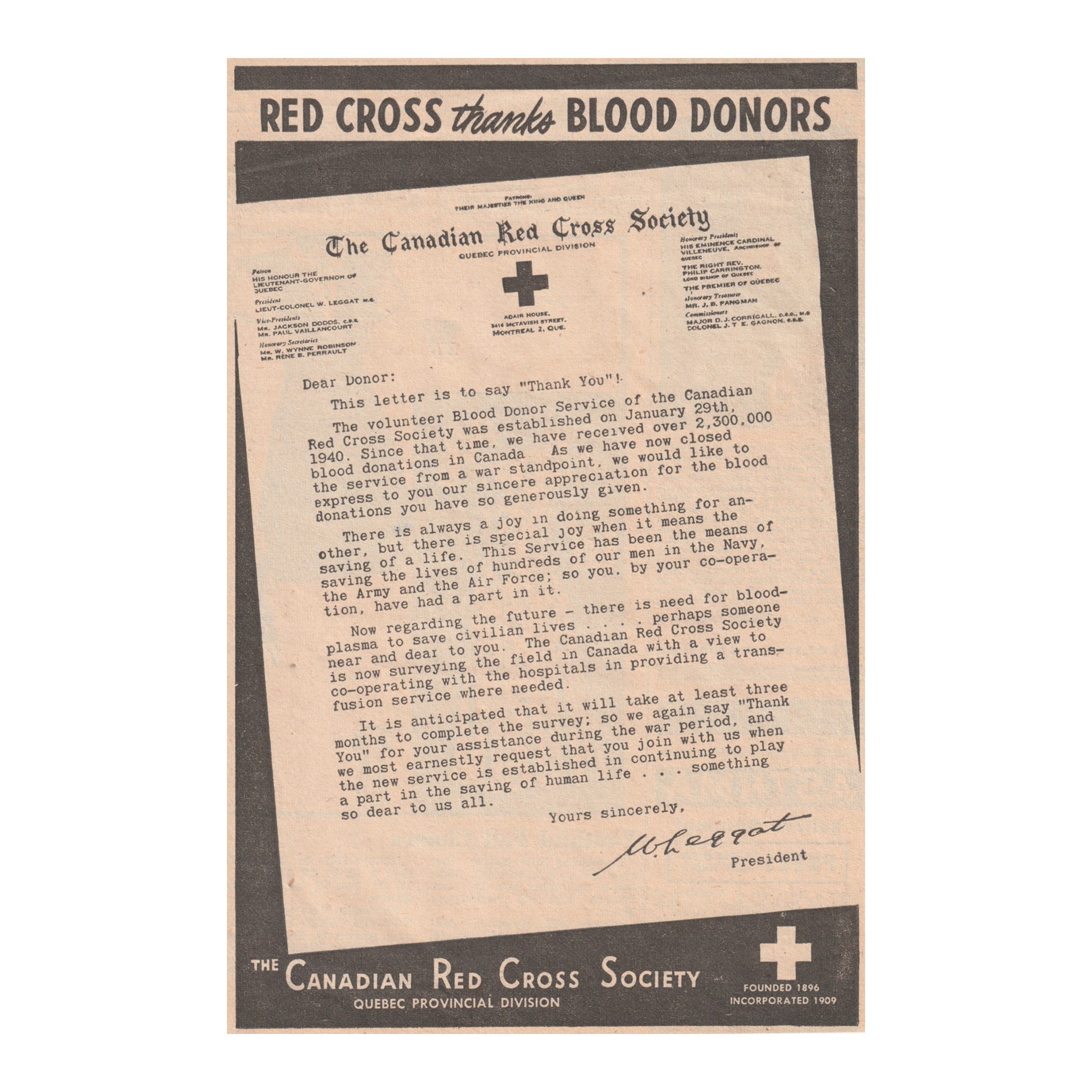
Figure 5. A 1945 newsprint ad thanking the volunteer donors who supported the Canadian Armed Forces and looking to the future of the establishment of a peacetime blood transfusion service.
Image from the collection of Dr. Jean Wang, shared with her permission.
At the end of World War II, the wartime blood donor program was discontinued but a nation-wide Blood Transfusion Service was reinstituted between 1947–1948 by the Canadian Red Cross Society (see Figure 5).
Since then, the blood system has continued to evolve, attempting to better understand and improve the donor experience in addition to modernizing the screening processes to ensure the quality and safety of the blood and blood products. For more information on current practices in donor selection and testing, refer to Chapter 6.
Global differences in access to a safe and secure blood supply
In 2018, more than 118 million donations of blood, including 106 million whole blood and 12 million apheresis donations, were made worldwide8 and 89% of these donations were from voluntary non-renumerated donors.8 However, the World Health Organization (WHO) also describes inequities between high- and lower-income countries, highlighting a lack of access to a safe and secure blood supply for at least 50% of the world’s population. As per this report, Canada was categorized as a high-income country. Approximately 40% of global blood donations are collected in high-income countries that account for 16% of the global population. In contrast, countries classified as lower-middle income or low income by WHO collect approximately 25% of the global donations and serve approximately 50% of the global population.8 Outside of North America, every region in the world demonstrated an increase in blood collections between 2008 to 2018, mainly because of increased voluntary non-renumerated donations.
Donors registered as female accounted for 33% of global donations, with the Americas reporting the highest proportion of donations by female donors (40%) and the Eastern Mediterranean reporting the lowest proportion (6%).8 Donations from repeat voluntary non-renumerated donors also varied widely across the 6 regions described in the WHO report, from 20% in Central and South America to 90% in Europe.
WHO also collected data in broad categories about donor deferral. Among the regions with donor selection criteria and procedures, the proportion of donors deferred ranged from 6.3% in Africa to 11.3% in Europe and 20.3% in the Americas. The majority of deferrals for donors in high- and middle-income countries resulted when donors did not meet the hemoglobin criteria. In high-income countries, travel history was the second most common cause for deferral, while in the upper-middle-income countries, “behaviours that can increase the chances of acquiring transmissible infections” was the second most common cause for deferral. For low-income countries, donors not meeting the weight criteria was the main reasons for donor deferral, followed by low hemoglobin.
In summary, between 2008 to 2018, there has been a rise in blood donations across the globe with major challenges encountered in lower-income regions that support the majority of the human population. Inadequate hemoglobin level is the most common cause of deferral from blood donation worldwide and highlights the importance of iron management and nutrition in donors.
Donor perspectives on blood and plasma donation
Donor perceptions of the health-related impact of donation
There is an increasing amount of social science research addressing motivations and barriers to blood9 and plasma donation10 and the broader theoretical concepts such as fairness, reciprocity, equity, warm glow,11 prosociality,12 and altruism.13 Though few studies have sought to understand donors’ perceptions of the health-related impacts of donation a systematic review found that donors and non-donors who hold negative beliefs about the health effects of donation, report concerns related to increases in the risk of infectious diseases, reduced vitality, vasovagal reactions and low iron levels.14 However, this area is under-researched, and thus it is not clear whether these perceptions inform decisions about donation.14 There is also some literature on donor-related activities that promote the well-being of blood donors by integrating health promotion initiatives and early detection of health issues.15, 16 This area is also under-researched, and it is not clear if this kind of activity motivates donation. A broader examination of the literature on the social science of donation can offer insight into the motivations and experiences of blood and plasma donors and demonstrate how donation is part of a broader social experience that is not limited to health outcomes.
Societal-level influences
While much of the field of the social science of blood donation has focused on individual-level factors related to motivations, deterrents, and experiences, more recent work has explored how contextual factors of specific settings inform donor experience. Similarly, the literature on plasma donation has focused on individual-level factors related to converting whole blood donors to plasma donors. This has resulted in a call for research into the factors that attract non-whole blood donors to become plasma donors, with a focus on broader social-level influences.10
Broader societal-level influences include exploring questions related to the social, political, and economic contexts (i.e., the economy, social justice movements, effects of a global pandemic); institutional contexts (i.e., how blood services operate in broader public health systems, shifting regulatory regime that exists for blood products, science/innovation system in universities and funding systems); organizational contexts (i.e., deferral policies and donor centre locations); and the context of a person’s everyday life (e.g., community of ethnic ancestry, work, education, family and culture). Each of these contextual factors can operate together and overlap.
One example of such work is the study of groups who have been historically marginalized and donor eligibility criteria. In some cases, these studies are undertaken specifically in response to social movements that seek to address marginalization or discrimination, and they involve deferral criteria that were originally designed to ensure the safety of the of transfusion of blood products.17-19 There is also an emerging body of research addressing organizational changes to the blood system to be more inclusive for all, such as work with gender diverse20, 21 and racialized people.22
Research has identified a variety of barriers to blood donation among racialized people. For example, a study of Black communities in Montreal indicated that a lack of trust and perceived social exclusion were barriers while the deep desire to help family and community were motivators related to donation.23 These findings resonated in a more recent study by Haw and colleagues which revealed multiple levels of interacting barriers to donation for donors of African ancestry in Canada, from systemic racism and mistrust of the health-care system to a lack of information about the blood donation process.22 While a variety of barriers have been identified, there is still more work to be done to discover, address and implement strategies to break down the remaining barriers related to blood donation that impact equity deserving groups.
Contextual factors that have been explored in relation to plasma donation include the investigation of assumptions related to payment for plasma and the role of the commercial sector in plasma manufacturing.24, 25 A study of plasma donors living in Canada revealed that some donors are opposed to commercial plasma collection in Canada because they believe it could undermine Canada’s public health-care system.24 In Canada, research has also found that plasma centre staff (nurses and phlebotomists) are critical to creating a donation experience that encourages retention26 and highlights the importance of staff input in creating the best donation experience.27
Thus, future work on specific populations and their interaction with various levels of social, political, cultural context can yield insights into donor behaviours, experiences and motivations. Perhaps the most pressing issue for this field is that the majority of the population does not donate. Thus, scholars in this field are turning to innovative approaches to research such as community-based participatory research, to gain a deeper more nuanced understanding of populations that do not donate, as well as to understand how societal shifts can impact perceptions of donation.
While the health-related impact of donation is currently under-studied, there is a growing body of literature situating donation experiences within broader societal level influences. These influences are intertwined with health systems and public health in general, and thus this connection between donation and donor wellness is an important topic for future research.
Donor screening policies and their impact on equity deserving groups
There is also a growing focus on understanding how donor screening policies, initially designed to ensure blood system safety, impact equity deserving groups.17, 18, 28 This includes both exploring and implementing changes that will make the blood system more inclusive for all.
Historically, equity deserving groups such as the 2SLGBTQIA+ community21, 29 and people of diverse ethnicities22, 30, 31 have been impacted by donor screening policies. For example, in 1992 men who had sex with men since 1977 became ineligible to donate due to the rising risk of HIV, which was a new disease at the time. This screening policy prevented many people from the 2SLBGTQIA+ community from donating blood. In 2021, plasma donation criteria were changed allowing some bisexual, queer and other men who have sex with men to donate. In 2022 Canadian Blood Services’ screening process was changed and questions asking about sexual orientation were removed. These were replaced with questions about sexual behaviour which were used in all eligibility screenings regardless of sexual orientation or gender. This more inclusive approach to donor screening was the result of continued consultations with patient groups, advocacy from 2SLGBTQIA+ organizations, and Canadian and international research that demonstrated the change was safe and necessary. Read more about the Sexual behaviour-based screening here.
Possible health benefits of blood or plasma donation
Articles in the press on the health benefits of donations for donors have made headlines in the past. Unfortunately, many of the reported benefits are not supported by strong, published scientific data and can be misleading to donors.
Many studies have focused on the cardiovascular health benefits of blood donation. The hypothesis that frequent donations promote cardiovascular health in healthy donors through the prevention of iron overload and decreased blood viscosity is not supported by high-quality data.32, 33 Moreover, a systematic review showed no association between donation and improved cardiovascular health, with inconsistent findings among the highest-quality studies, none of which used a randomized designs.33 The major drawback of non-randomized studies is that they are unable to correct for the “healthy donor effect”, as donors are inherently healthy because of the rigorous donor screening process.33
An exception to this pertains to individuals living with hereditary hemochromatosis, which can predispose individuals to iron overload and potentially compromise cardiovascular health ( see Table 1). These individuals often require therapeutic phlebotomies (i.e., regular blood removal to intentionally deplete iron stores). Some people with hereditary hemochromatosis who meet the donor screening criteria can donate whole blood to maintain the benefits of phlebotomies.34 This should be done with the supervision of their physician, as the minimum inter-donation interval may not be sufficient to prevent iron overload. Similarly, other physiologic and disease states are associated with elevated red blood cell counts, but the role of blood donation in patient management is variable (Table 1).
Table 1. Conditions with increased red blood cell count (polycythemia) or iron and the role of blood donation in management.35
|
Condition |
Is the underlying illness a cause for donor deferral? | Does evidence support the use of phlebotomies in some cases? |
|---|---|---|
| Hereditary hemochromatosis | No | Yes |
| Chronic hypoxemic state from obstructive sleep apnea | No | No |
| Chronic hypoxemic state from some lung and heart diseases | Yes | No |
| Myeloproliferative disorders including polycythemia rubra vera | Yes | Yes |
| High affinity hemoglobin | Yes | Yes |
| Other: smoking, medication (i.e., erythropoietin/testosterone supplementation), high-altitude living | No | No |
| Some cancers | Yes | No |
For plasma donors, no studies have demonstrated health benefit from donation. Post-donation, an acute and temporary decrease in circulating cholesterol levels and blood pressure does not have a lasting impact on long-term cardiovascular health.36, 37
Moreover, some believe that donors benefit from a physical exam at the time of donation. The donor screening questionnaire and blood tests performed in donation centres should not be considered equivalent to a comprehensive or preventative health screen, as the screening process only evaluates eligibility to donate. A complete set of vital signs is not routinely required, nor is a physical examination, and donors undergo a limited assessment of the skin/vein site where the phlebotomy is being performed.
Donors are tested before donation to ensure their hemoglobin is high enough for donation and donor samples are also tested after donation for blood typing and screening of specific infectious agents. To read more on donor selection and testing, refer to Chapter 6 of the Clinical Guide to Transfusion and the Canadian Blood Services’ annual Surveillance Report. For select donors, a ferritin level is also measured to assess iron stores and a platelet count is measured in apheresis platelet donors.
Donors may learn new information from the report of any abnormal or indeterminate findings occurring during donor screening and blood operators usually provide a written description of the abnormal findings/results and recommend that donors seek medical attention for additional management. Donors are also informed if they are found to have a rare blood group. For the donors, information regarding a rare blood group can be important for awareness through a future pregnancy or situations where they may require transfusions.
Voluntarily donating blood is an act of benevolence and studies have shown that donating blood can generate positive emotions also referred to by some as the “warm glow” effect.38 However, the impact of this emotional well-being on donor health outcomes and longevity has not been studied.
Adverse events in whole blood donors
Some adverse events of donations are common to both whole blood and apheresis donation procedures;39 with more data available from studies of whole blood donation. More information on the types of donations can be found in Chapter 2 and Chapter 18 of the Clinical Guide to Transfusion. Adverse events occurring with donation procedures may include vasovagal reactions, bruising and hematomas, nerve injury, local allergic reactions, localized inflammation, iron deficiency and major adverse cardiovascular events (MACE). The overall moderate to severe adverse event risk with whole blood donation is 0.49%.40 The rate of adverse reactions are higher amongst first-time, younger and female donors.41 These unique considerations and factors related to adverse reactions during whole blood and apheresis donations are discussed below (see Table 2 for a summary of adverse reactions associated with whole blood donation).
Table 2. Whole blood donation-associated donor adverse events and their frequency.†
| Reaction | Definition | Frequency (per 10,000 donations)39 |
Frequency of reaction causing donation failure40 |
|---|---|---|---|
| Vasovagal event | Pre-syncope or syncope | 0.014% | |
| Mild | No LOC (loss of consciousness) | 1.63 | |
| Moderate | LOC < 60 seconds and no complications | 0.27 | |
| Severe | LOC ≥ 60 seconds with or without loss of bladder/bowel control or injury | 0.05 | |
| Major cardiovascular event | Acute cardiac symptoms, myocardial infarction, cardiac arrest, transient ischemic attack, cerebrovascular accident, death within 24 hours of donation (may or may not be related to donation) | 0.005 - 0.01 | N/A |
| Arterial puncture | Needle inserted into artery instead of vein | 0.3 | 0.0016% |
| Bruising/hematoma | Skin discolouration because of blood leakage from blood vessel at time of phlebotomy | 8.7 | 0.271% |
| Re-bleed | Bleeding from phlebotomy site after donation | 0.11 | N/A |
| Nerve injury | Needle irritation or injury of nerve during phlebotomy | 0.2 | N/A |
| Immediate | Immediately after or during phlebotomy | ||
| Prolonged | Lasting ≥ 1 year after donation | ||
| Inflammation or infection | Redness or infection at needle sites, usually several days after donation | 0.03 | N/A |
| Local allergic reactions | Rash from skin cleaning solution or dressing | 0.03 | N/A |
| Arm pain | Pain because of blood pressure cuff, tourniquet or arm position | 0.29 | N/A |
| †Some donation related adverse reaction rates are higher in first-time donors, donors registered as female, and younger donors, such as vasovagal reactions. These are discussed in text below. | |||
Vasovagal reactions
A vasovagal reaction is defined by the International Society of Blood Transfusion as a general feeling of discomfort and weakness with anxiety, dizziness and nausea, which may progress to loss of consciousness.43 It can be considered:
- Mild when not associated with a loss of consciousness episode
- Moderate if the loss of consciousness lasts < 60 seconds without complications
- Severe if the loss of consciousness lasts at least 60 seconds or results in injury/complications such as loss of bowel/bladder function
Vasovagal reactions most commonly occur during or immediately after donation at the collection site but may also be delayed.
A mild vasovagal reaction is the most common adverse event in donors. Although more frequently observed with whole blood donations, vasovagal reactions also occur following apheresis donations.43 Risk factors for vasovagal reactions in donors include less than 25 years of age, female sex, first-time donor status, and low estimated blood volume. Other risk factors are listed in Table 3.42
Table 3. Risk factors and relative risk (if known) for vasovagal reactions (VVRs) for whole blood donations (adapted from Thijsen & Masser42).
| Observable donor characteristics | Unobservable donor characteristics | Contextual factors |
|---|---|---|
|
Mitigation strategies to minimize the risk of vasovagal reactions for whole blood donation include pre-donation water and salty snacks, which have been associated with a 15% reduction in vasovagal reactions.48, 49 Other potential mitigation strategies are detailed in Table 4.48
Table 4. Effectiveness of vasovagal reaction (VVR) mitigation strategies for whole blood donation.50
| Vasovagal reaction (VVR) mitigation strategy |
Impact on VVR |
|---|---|
| Peri-donation water intake | Intake of 330 mL to 500 mL water or isotonic solution has demonstrated reduction in vasovagal reaction rate with odds ratio = 0.74. |
| Applied muscle tension (AMT) |
Unclear impact of this method as it is poorly standardized across studies. AMT was associated with variable impact on phlebotomist- and patient-reported VVR and VVR severity in the literature. |
| Water loading, salty snack and AMT | Salty snacks in combination with water loading and AMT have shown decreased rates of vasovagal reactions with loss of consciousness by 25%. |
| Social support | Being accompanied by someone trained to provide support and be reassuring reduced vasovagal reactions in donors with a history of < 3 donations and increased the likelihood of donating again the following year. |
| Fear assessment pre-donation in combination with a brochure summarizing evidence-based methods to improve stress-induced adverse events and a tailored conversation about strategies to reduce donor fear | This method was shown to improve the perception of support which was associated with less venipuncture pain. Venipuncture pain was shown to be associated with more self-reported VVR. |
| Distraction such as focusing on non-donating arm | Distractions were shown to enhance the effect of AMT. |
| Breathing techniques | Breathing techniques were shown to be beneficial for donors who had low-fear levels. |
Local allergic reactions
A local allergic reaction is defined as red or irritated skin at the site of venipuncture.43 It can be caused by products used for disinfection such as chlorhexidine, adhesive bandages, or latex exposure. The reaction can be limited to the venipuncture site or involve a bigger area of the arm. The reaction can be immediate or delayed following donation. At most donation centres, donors can usually request an alternative disinfectant or bandages to prevent an allergic reaction.
Localized inflammation
Localized inflammation of the venipuncture site can be attributed to thrombophlebitis or cellulitis. Thrombophlebitis can be provoked by trauma and inflammation of the involved vein and manifests with redness, swelling and tenderness along the vein. Cellulitis may result from inadequate sterilization of the venipuncture site and symptoms include redness, swelling and tenderness around the venipuncture site, but not localized to the vein.43
Bruising/hematomas and arterial puncture
Bruising and hematomas are common adverse events of both whole blood and apheresis donations. They are the result of blood extravasation from the venipuncture site and in most cases cause no additional complication.
Rarely, a hematoma can develop from an accidental arterial puncture during the attempted venipuncture. Arterial punctures require prolonged puncture site compression to prevent the formation of a large hematoma and compartment syndrome. While bruising is a common adverse event, arterial punctures are rare.
Nerve injury/irritation
Nerve injury and irritation may be a cause of prolonged arm pain following phlebotomy. Nerves often depend on their proximity to blood vessels for passive nutrient supply. A proportion of the population has nerves intertwined or overlying blood vessels in the antecubital fossa, thus exposing the nerve to direct injury during phlebotomy without evidence of trauma or inadequate phlebotomy technique. Cutaneous branches of the median or radial nerves are commonly thought to be involved.51 Risk factors for nerve injury include the donor’s anatomy and the size of the phlebotomy needle. Most often, the damage is limited to the myelin sheath of the nerve, which acts as the outer protecting and isolating layer of the nerve itself. This is called neuropraxia and is associated with rapid recovery of symptoms. Axonal damage without connective tissue damage, also called axonotmesis, is caused by a more severe injury to both the myelin sheath and the nerve itself without complete severing of the nerve. Neurotmesis, the most severe form of nerve damage, refers to cases where the nerve is completely severed.51 When axonal damage occurs, the distal end of the neuron undergoes degeneration from macrophages, a process called Wallerian degeneration. Conversely, the proximal segment undergoes retrograde degenerative changes, followed by a process of regeneration. However, the process of regeneration can be long as axons grow at a speed of 1 to 2 mm/day.52 For this reason, symptoms following axonal damage can take months to heal, with 70%, 93% and 96% of the damage resolving within 1, 3 and 6 months, respectively.51 In 1 case per 1.5 million donors, nerve damage results in chronic symptoms. Damage to C-nociceptor fibres causes burning and lancinating pains, whereas damage to the sensory A-beta and A-delta fibres causes paresthesia and dysesthesia. Symptom management can be challenging.52 Both vitamin B12 and folate supplementation are important for myelin sheath formation. Animal studies on non-steroidal anti-inflammatory drugs showed enhanced axon growth and remyelination and can be considered in donors with nerve injury.52
Major adverse cardiovascular events (MACE)
MACE is defined as myocardial infarction, cardiac arrest, other acute cardiac symptoms, transient ischemic attack, cerebrovascular accident or death within 24 hours after blood donation.43MACE are exceedingly rare and reported in 0.01 and 0.05 of 100,000 whole blood and apheresis donors, respectively.41 In addition, demonstrating the imputability of the donation in cases of MACE is often challenging. The donor screening questionnaire plays an important role in identifying people at risk of MACE and deferring them from donating.
Iron deficiency
Iron deficiency is a common nutritional deficiency in the general population which can be further exacerbated by blood donation. Although often underrecognized,53-55 iron deficiency without anemia (IDWA) is common among blood donors.56 Up to 35% of whole blood donors become iron deficient from regular whole blood donation.57 Each whole blood donation contains 225 mg to 250 mg of iron. Donor characteristics impacting iron stores have been studied by blood operators in Canada, the US, Australia, Switzerland, the Netherlands and beyond.58-65 Younger donors (especially those aged < 25 years) and those registered as female or making 2 or more donations per year are at the highest risk of becoming iron deficient after whole blood donations.58, 63-66 Notifying donors about their iron deficiency as well as providing iron supplementation can be effective.66, 67
Currently, most blood operators use a fingerstick capillary blood hemoglobin test to ensure potential donors meet the minimum eligibility requirement for hemoglobin threshold to donate. The hemoglobin threshold to donate varies across blood operators. In Canada, for whole blood donation, the hemoglobin threshold is 125 g/L for female and 130 g/L for male donors, which is greater than levels considered to indicate clinical anemia. Not meeting the hemoglobin threshold is the most common cause of deferral for otherwise healthy blood donors. In most whole blood donors who do not meet the hemoglobin threshold, low iron stores remain the most common cause. However, iron stores are often depleted before an individual experiences a decline in their hemoglobin levels. In fact, donors with a hemoglobin of less than 130 g/L and ferritin less than 10 µg/L have a specificity of 96% predicting the donor will not meet hemoglobin criteria at subsequent visits.68 This testing does not account for other important factors that independently affect hemoglobin levels, such as thalassemia trait or vitamin B12 deficiency.
To better test iron stores, the use of selective ferritin testing is slowly expanding among blood operators internationally. Canadian Blood Services initiated ferritin testing in select donors at the highest risk of developing iron deficiency in January 2023.
IDWA can cause fatigue, decreased exercise capacity, neurocognitive changes, pica, restless leg syndrome, and impaired quality of life.69-74 IDWA can progress to iron-deficiency anemia if left untreated. The physiological manifestations of iron-deficiency anemia include reduced immune function, impaired cognitive performance, behaviour changes, decreased thermoregulatory performance and energy metabolism, and diminished exercise capacity.75, 76
Iron deficiency from donation can be prevented. The various mitigation strategies are described in Table 5.
Table 5. Iron deficiency mitigation strategies for whole blood donors.
| Iron deficiency mitigation considerations | Higher risk group | Strategies used by blood operators |
|---|---|---|
| Donor eligibility criteria | ||
| Age | Donors aged < 25 years | Modify the frequency of donation for younger donors. |
| Gender | Donors registered as female | Modify inter-donation intervals to allow a longer time frame between donations to help replete iron stores. Use different hemoglobin thresholds according to sex if ferritin testing is not available. |
| Frequency of donation | Repeat donors, especially those with ≥ 2 donations per year | Adapted donation frequency to ensure donors have sufficient iron stores and there is a sustainable blood supply available. Frequent donors may need additional considerations such as closer monitoring of ferritin levels, increasing reminders for iron supplementation if safe, etc. |
| Donor testing | ||
| Hemoglobin level | Those with hemoglobin that is progressively declining or those who do not meet the minimal threshold to donate are likely iron deficient | A subgroup of donors may require additional collaboration to ensure more attention to iron monitoring and repletion and decreased donation frequency. |
| Ferritin level | Those with a ferritin level ≤ 25 mcg/L | This subgroup of donors may benefit from decreased donation frequency and iron repletion. |
To replace one whole blood donation,77 daily elemental iron supplementation of 37.5 mg for at least 8 weeks is required. Donors who take at least 37.5 mg of elemental iron supplementation return to their pre-donation hemoglobin levels approximately 3 to 5 times faster.78 For individuals donating on a regular basis, particularly in individuals who are menstruating or have had a recent pregnancy, it is very difficult to replace the amount of iron lost through donation by diet or multivitamins alone; multivitamins do not contain sufficient amounts of iron for replenishment.79
Health-care practitioners further assessing donors found to have low hemoglobin or ferritin levels may repeat measurements on a venous sample. Additional testing is based on a variety of factors such as the patient’s age, menstrual status, pregnancy history, family history of gastrointestinal cancer, and the presence of any signs or symptoms of other possible underlying conditions contributing to blood loss or impaired nutrient absorption. Guidelines developed by the British Society of Gastroenterology recommend obtaining a history of blood donation as part of the investigation of iron deficiency.80
Adverse events in apheresis donors
Apheresis donations take longer than whole blood donations and have a return phase that exposes the donor to additional saline and citrate. As a result, some adverse events are specific to the apheresis procedure: citrate reactions (hypocalcemia), tissue infiltration and compartment syndrome, allergic reactions, and air embolism (Table 6). Other theoretical long-term effects of apheresis donations will also be discussed.
Table 6. Apheresis-associated adverse donor reactions and their frequency.†,81
| Reaction | Definition | Frequency (per 10,000 donations)39 |
|---|---|---|
| Bruising/hematoma | Skin discolouration because of blood leakage from blood vessel at time of phlebotomy | 15.9 |
| Citrate reaction | Neuromuscular hyperactivity related to reduced ionized calcium levels | 7.1 |
| Arm pain | Pain because of blood pressure cuff, tourniquet or arm position | 0.44 |
| Vasovagal event |
Pre-syncope or syncope |
|
| Mild | No loss of consciousness (LOC) | 0.61 |
| Moderate | LOC < 60 seconds and no complications | 0.10 |
| Severe | LOC ≥ 60 seconds without loss of bladder/bowel control or injury | 0.005 |
| Infiltration | Intravenous solute enters extravascular tissues during volume replacement (generally only in double red blood cell procedures) | 0.22 |
| Nerve injury | Needle irritation or injury of nerve during phlebotomy | 0.19 |
| Arterial puncture | Needle inserted into artery instead of vein | 0.16 |
| Inflammation or infection | Redness or infection at needle sites, usually several days after donation | 0.07 |
| Re-bleed | Bleeding from phlebotomy site after donation | 0.06 |
| Major cardiovascular event | Acute cardiac symptoms, myocardial infarction, cardiac arrest, transient ischemic attack, cerebrovascular accident or death within 24 hours of donation (may or may not be related to donation) | 0.05 |
| Local allergic reactions | Rash from skin cleaning solution or dressing | 0.04 |
| Anaphylaxis | Severe systemic allergic reaction (2 systems involved) | 0.04 |
| Hemolysis | Damage to donor cells (valves/tubing obstruction/incorrect installation) and release of free hemoglobin | 0 |
| Air embolism | Air bubble introduced into donor's circulation | 0 |
†Some donation related adverse reaction rates are higher in first-time donors, donors registered as female, and younger donors, such as vasovagal reactions. These are discussed in text below.
Vasovagal reactions
Vasovagal reactions are less frequent with apheresis procedures compared to whole blood donations.39 However, even mild reactions deter donors from returning. Hence, it is vital to understand who may be at higher risk of vasovagal reactions and institute preventative strategies.
Important factors known to increase the risk of vasovagal reactions include:39, 81-83
- Donor inexperience (first-time donation without prior whole blood experience)
- Younger age, especially age < 25 years
- Female sex
- Needle or donation fear
- Total blood volume < 3.5 L
- Collection volumes > 18% total estimated blood volume
Some vasovagal reactions may be prevented with appropriate donor screening, care and counselling. Most vasovagal mitigation strategies are better studied in whole blood donors and have been adopted into apheresis donor management including a minimum age cut-off for donation, applied muscle tension and intake of peri-donation water and salty snack. Additional strategies that help reduce the risk of vasovagal reactions include:83-85
- A minimum height and weight criteria ensuring the total blood volume of the donor is ≥ 3.5 L.
- Plasmapheresis collection volume determined based on percentage of total blood volume; for instance, collecting first at lower volumes (approximately 16% of total blood volume) and then progressing to a pre-set maximum of approximately 18% total blood volume.
- Performing a saline replacement to help minimize volume loss during or after the procedure.
Most blood operators incorporate careful donor screening, collection protocols and counselling to help minimize vasovagal reaction risks and maintain donor well-being. being.
Citrate reactions
Citrate is the anticoagulant used in apheresis circuits and works through reversible chelation of calcium.86 Depending on the volume of return as well as length of the procedure, apheresis donors are infused with a variable amount of citrate. In healthy individuals, an estimated 3 g of citrate can be metabolized by the body every 5 minutes.87 Following an apheresis procedure, citrate is fully metabolized within 4 hours. Excessive citrate leads to symptomatic hypocalcemia when there is a drop in ionized calcium concentration of 20% to 35%.87
Hypocalcemia-related symptoms based on their degree of severity are shown in Table 7. As donors are healthy and symptoms of citrate toxicity are carefully monitored, such complications are infrequent and reported in 1.2% of donors.86 Citrate toxicity has been reported more frequently in plateletpheresis than in plasmapheresis because of the longer duration of the plateletpheresis process. Oral calcium is commonly provided during apheresis collections to help mitigate citrate reactions.
The management of citrate reactions depends on the severity of the symptoms. In most cases, the rate of flow can be slowed down and the blood-to-citrate ratio increased. Oral or intravenous calcium can be administered depending on the severity of symptoms and the procedure can be paused.88
Table 7. Symptoms of citrate toxicity.86
| Mild | Moderate | Severe |
|---|---|---|
|
|
|
Infiltration
Infiltration during apheresis donations occurs when reinfused fluid and uncollected blood components leak into the soft tissue during the return phase of the procedure because of a dislodged needle. Typical findings that suggest fluid extravasation include poor blood flow through the venous access, swelling, pressure and pain. A hematoma may form with the return of red blood cells. While small infiltrations are benign, larger and deeper accumulations of fluid and blood may cause compression of blood vessels, nerves, and tissues. In extreme situations, this may lead to compartment syndrome and irreversible nerve and tissue damage. As apheresis procedures are closely monitored, infiltration is exceedingly rare.
Air embolism
Air embolism is a rare but severe complication of apheresis donations. As a result of improper priming of the lines, defective kits or incorrect manipulation of the tubing, air bubbles can be inadvertently injected into the donor during the return phase of the procedure. Air bubbles in the venous circulation can travel to the pulmonary vasculature and may cause vessel obstruction. In many cases, the small volume of injected air is rapidly dissolved in the blood. It is estimated that 3 to 8 mL/kg of air is necessary to cause a clinically significant air embolism. Symptoms include dyspnea, hypoxemia, tachycardia, and hypotension.88 Immediate recognition of this complication is important as positioning the donor in the Trendelenburg and left lateral decubitus positions will help dislodge the air bubbles, which will travel back into the right heart ventricle. New air-sensing technology incorporated into apheresis machines has significantly reduced the risks of air embolism by stopping the circuit upon detection of bubbles.88
Severe allergic reactions
Severe systemic allergic reactions are reported in 0.04 of 10,000 donations.39 While rates are now low, severe hypersensitivity reactions were reported in 1% of plateletpheresis donors in 1986.89 Some of the affected donors have evidence of ethylene oxide gas hypersensitivity. Ethylene oxide has been used to sterilize the plastic circuit of the disposable apheresis and hemodialysis kits and remains in use to this day given its effectiveness and overall safety profile (Standard for Surveillance of Complications Related to Blood Donation, AABB).90-92
Lymphopenia
Following the report of an incidental finding of lymphopenia in plateletpheresis donors, Gansner et al.93 demonstrated that frequent plateletpheresis is associated with lymphopenia of both CD4+ and CD8+ lymphocytes in many donors. In fact, the apheresis circuit includes a leukoreduction system chamber that captures and discards circulating white cells such as lymphocytes. Of 20 recurrent donors who contribute 20 to 24 donations per year, a CD4+ lymphocyte count less than or equal to 200 cells/mL was identified in 6 donors (30%) and low CD8+ lymphocyte counts in 11 donors (55%). A loss of up to 10% of circulating CD4+ lymphocytes per donation can be expected. However, this finding was not associated with adverse events or opportunistic infection in donors.94 In fact, most lymphocytes reside in lymphoid tissue rather than in the circulation.93 Moreover, some leukodepletion can be prevented with a process called rinse-back where saline is used to return the residual cells from the tubing in the machine. This procedure is routinely performed at Canadian Blood Services. Lymphopenia secondary to frequent apheresis donations is not a contraindication for donation.
Hypogammaglobulinemia
Historical data, originally collected in undernourished incarcerated individuals donating high volumes at higher frequencies, indicated that apheresis may lead to clinically meaningful decreases in immunoglobulin levels.95-97 However, current practices of plasmapheresis have not reproduced these findings nor suggested an impact on humoral immunity.
In 1991, a 10-year Canadian study of 208 donors with more than 18,000 plasmapheresis donations showed no difference in the IgG, IgM, or total serum protein levels or albumin concentration.98 An additional 60 Canadian donors were studied and demonstrated slightly lower total protein and IgG levels when donating up to 600 mL weekly when compared with a longer transfusion interval of 14 days or more. However, all protein levels remained within the normal range.99Moreover, the decrease in the total protein levels was seen during the first 3 months, with subsequent stabilization or increase in donors’ baseline levels.99
In individuals donating large volumes of plasma frequently, including up to 180 donations per year, 850 mL/donation and inter-donation intervals as short as 72 hours, no significant decrease in protein levels was seen over 3 years of observation. The total serum protein, albumin, and IgG levels at baseline and at multiple donation intervals over the observation period remained within the normal range even after 30 to 60 donations.100 Another cross-sectional study demonstrated no impairment in humoral and cellular immunity among 483 high-intensity donors donating up to 45 L of plasma per year compared to healthy non-donor controls over a 36-month period.101
In summary, frequent and high-volume plasmapheresis has not demonstrated clinically significant hypogammaglobulinemia or impairment of humoral immunity.
Osteoporosis and chronic citrate exposure
Plasma and platelet donations by apheresis can be repeated every 6 and 14 days, respectively. Given the chronic exposure to citrate in recurrent donors, there is a theoretical concern for loss of bone density, particularly in patients at increased risk of osteoporosis. Indeed, citrate-induced hypocalcemia activates the parathyroid, causing release of parathyroid hormone, promoting calcium liberation from the bone matrix. For this reason, some blood operators may defer donors from apheresis donations if they have a history of pathological fractures or osteoporosis. However, there is a paucity of data to support this practice. The randomized ALTRUYST study, published in 2018, failed to identify a detrimental impact on bone mineral density in healthy subjects with a normal bone mineral density who made at least 20 platelet donations in the previous year.102 The retrospective SCANDAT2 database demonstrated no association between donation frequency and the risk of fractures among 140,289 apheresis donors.103
Donor testing and deferral risk
Testing for transfusion-transmitted infection: donor management
Many serological tests are performed on each donation to ensure the blood is safe for donation. These include screening for transfusion-transmissible infections, blood group determination, and antibody detection. Refer to Chapter 6 of this Guide for information about the screening tests performed on blood donations at Canadian Blood Services. A positive test result may result in the unit being discarded, and the donor may be temporarily or indefinitely deferred from all or some forms of donation. For donors, the impact of receiving these test results can be significant, as it may generate anxiety, confusion and frustration. The following section explains what leads to these deferrals and how Canadian Blood Services guides donors toward seeking medical attention if appropriate or toward other types of blood donation when possible.
Infectious serological tests must be negative to label a blood product. The blood operator is responsible for using the appropriate Health Canada–approved screening tests as described in Chapter 6 of this Guide. As blood donors are healthy and screened for risk factors for transfusion-transmissible infection, they have a low pre-test probability of having an infection. In this setting, highly sensitive serological screening tests maximize the detection rate at the cost of a higher false-positive rate and may not be the same assays as used for diagnostic purposes in the clinical setting. All donors whose donations test reactive using these highly sensitive serological screening tests are deferred from donation whether an actual illness is later confirmed or not. The higher false-positive rate is accepted as a precautionary step to prevent the introduction of a pathogen into the blood supply.
Canadian Blood Services will perform a more specific confirmatory test on the donation when screening results are repeat reactive to support blood donor counselling. When the screening test is positive, but the confirmatory assay is negative or indeterminate, a letter is sent to the donor. This letter informs the donor to seek medical attention to confirm the findings with the appropriate blood test and provides answers to frequently asked donor questions. When the confirmatory test result is positive, public health is informed when appropriate and the donor is contacted directly.
Those donors whose donations test false reactive may return for re-testing as part of the re-entry program. Alternative testing assays that may be used for re-entry must also be Health Canada approved for blood product labelling
Testing for blood group and antibody detection: donor management
The non-infectious serological tests performed on blood donations include a direct antiglobulin test, antibody identification, and ABO/RhD typing (refer to Chapter 6 of this Guide for more information on blood group determination and antibody detection). Donors with a positive direct antiglobulin test are deferred from donating red blood cells to avoid interference in the blood banks when units are crossmatched and referred toward apheresis donation even though the unit itself would not necessarily cause harm to the recipient. Those with identified alloantibodies are deferred from donating plasma-containing products, but red blood cell donations are permitted given the low plasma content of red blood cell units. In determining the blood type, any ABO discrepancy is further investigated and most causes of ABO discrepancy mandate donor deferral. Donors with the subgroups A2, A3, and B3 are not deferred if they do not have detectable anti-A1. Lastly, all donors with lower strength reactions during D typing undergo RhD genotyping. Those with mutations of the D antigen are deferred from donating red blood cells. Donors are informed whether they should be considered as RhD positive or negative.
Conclusion
The quality of the relationship between Canadian Blood Services and donors is essential to the national blood supply system, and as a part of this relationship, Canadian Blood Services values the well-being and health of its donors. While it may be challenging for donors to be informed of the possibility a transfusion-transmittable infection detected in their donation or that they can no longer donate because of serological test results, Canadian Blood Services aims to help donors seek medical help when needed, provide information to help guide and inform donors, and offer alternative donation options when possible.
Practice questions
Below are two sets of knowledge check questions hosted on Microsoft forms. These questions are designed to help reinforce key concepts and support your learning. Your responses will be anonymous, and scores for this learning assessment will be presented to you for self-assessment purposes. These scores and your answers will be recorded in Microsoft Forms and will be used to assess the impact of knowledge check questions as an additional educational resource in the Clinical Guide to Transfusion for quality improvement of this resource.
If you have any questions about these practice questions or suggestions for improvement, please contact us through the Feedback form.
If you are an educator and would like to use these questions in your teaching, please acknowledge Canadian Blood Services.
Knowledge-based questions
Case-based questions
Continuing professional development credits
Fellows and health-care professionals who participate in the Canadian Royal College's Maintenance of Certification (MOC) program can claim the reading of the Clinical Guide to Transfusion as a continuing professional development (CPD) activity under Section 2: Individual learning. Learners can claim 0.5 credits per hour of reading to a maximum of 30 credits per year.
Medical laboratory technologists who participate in the Canadian Society for Medical Laboratory Sciences’ Professional Enhancement Program (PEP) can claim the reading of the Clinical Guide to Transfusion as a non-verified activity.
Acknowledgements
The authors acknowledge Dr. Catherine Latour and Catherine Thibeault of Héma-Québec, as well as Dr. Mindy Goldman, Dr. Michelle Zeller, Dr. Matthew Yan, and Mx. Terrie Foster of Canadian Blood Services, and Dr. Jean Wang of the University of Toronto for their review of this chapter.
Suggested citation
Bienz M, Holloway K, Khandelwal A. An overview of donor health, wellness and perspectives. In: Khandelwal A, Brooks K, editors. Clinical Guide to Transfusion [Internet]. Ottawa: Canadian Blood Services, YYYY [cited YYYY MM DD]. Chapter 21. Available from: https://professionaleducation.blood.ca
If you have questions about the Clinical Guide to Transfusion or suggestions for improvement, please contact us through the Feedback form.
References
- Wang, J. C. (2018). A Call to Arms: Wartime Blood Donor Recruitment. Transfus Med Rev, 32(1), 52-57. https://doi.org/10.1016/j.tmrv.2017.06.004
- Duran Jorda, F. (1939). THE BARCELONA BLOOD-TRANSFUSION SERVICE. The Lancet, 233(6031), 773-775. https://doi.org/10.1016/S0140-6736(00)60392-6
- The Centre for Blood Research. (2020, 2020-08-06). Dr. Norman Bethune – A leading figure in transfusion medicine. The Centre for Blood Research. Retrieved 2025-03-11 from https://cbr.ubc.ca/dr-norman-bethune-a-leading-figure-in-transfusion-medicine/
- Rawling, B. (2001). Providing the gift of life: Canadian medical practitioners and the treatment of shock on the battlefield. Canadian Military History, 10(1), 2.
- Tan, S. Y., & Merritt, C. (2017). Charles Richard Drew (1904-1950): Father of blood banking. Singapore Med J, 58(10), 593-594. https://doi.org/10.11622/smedj.2017099
- Drew, C. R. (1940). Banked blood: A study in blood preservation Columbia University]. http://resource.nlm.nih.gov/101584649X142
- Kapp, R. W. (1995). Charles H. Best, the Canadian Red Cross Society, and Canada's first national blood donation program. Canadian Bulletin of Medical History, 12(1), 27-46. https://doi.org/10.3138/cbmh.12.1.27
- Health Product Policy and Standards. (2021). Global status report on blood safety and availability 2021. World Health Organization. https://www.who.int/publications/i/item/9789240051683
- Piersma, T. W., Bekkers, R., Klinkenberg, E. F., De Kort, W., & Merz, E. M. (2017). Individual, contextual and network characteristics of blood donors and non-donors: a systematic review of recent literature. Blood Transfus, 15(5), 382-397. https://doi.org/10.2450/2017.0064-17
- Berger, M., Easterbrook, A., Holloway, K., Devine, D., & Bansback, N. (2023). What influences decisions to donate plasma? A rapid review of the literature. Vox Sang, 118(10), 817-824. https://doi.org/10.1111/vox.13496
- Ferguson, E. (2021). Strategies and theories to attract and retain blood donors: fairness, reciprocity, equity and warm‐glow. ISBT Science Series, 16(3), 219-225. https://doi.org/10.1111/voxs.12640
- Ferguson, E., & Masser, B. (2018). Emotions and Prosociality: Lessons for Blood Donation. In Williams, Rhodes and Conner (Eds.), Affective Determinants of Health Behaviour. Oxford University Press.
- Masser, B., Ferguson, E., Merz, E.-M., & Williams, L. (2020). Beyond Description: The Predictive Role of Affect, Memory, and Context in the Decision to Donate or Not Donate Blood. In (Vol. 2024).
- Thorpe, R., Masser, B., Coundouris, S. P., Hyde, M. K., Kruse, S. P., & Davison, T. E. (2024). The health impacts of blood donation: a systematic review of donor and non-donor perceptions. Blood Transfusion, 22(1), 7-19. https://doi.org/10.2450/BloodTransfus.494
- Shaz, B. H., Kessler, D., & Hillyer, C. D. (2012). Evaluating the role of blood collection centers in public health: a status report. Transfus Med Rev, 26(1), 58-67. https://doi.org/10.1016/j.tmrv.2011.07.002
- Marx, L. J. H., Van Walraven, S. M., van Zelm, R., & Sassen, B. (2025). Health promotion for blood donors: A scoping review. Public Health Pract (Oxf), 9, 100604. https://doi.org/10.1016/j.puhip.2025.100604
- Fisher, W. A., Kohut, T., Woo, H., & Haw, J. (2023). Alternatives to blood donor deferral of gay, bisexual, and other men who have sex with men: Acceptability of screening the sexual risk behavior of all blood donors. Transfusion, 63(3), 531-540. https://doi.org/10.1111/trf.17241
- Haw, J., Woo, H., Kohut, T., & Fisher, W. (2022). Sexual risk behavior questions: Understanding and mitigating donor discomfort. Transfusion, 62(2), 355-364. https://doi.org/10.1111/trf.16755
- Vesnaver, E., Butler-Foster, T., Goldman, M., Gibson, E., Palumbo, A., Lapierre, D., Hill, N. E., MacDonagh, R., Rubini, K. A., Bridel, W., Miguel, G., Rosser, A., MacPherson, P., Randall, T., Osbourne-Sorrell, W., O’Brien, S. F., Otis, J., Greaves, M., Al-Bakri, T. B., . . . Presseau, J. (2023). Improved access yet inequitable experience: gay, bisexual and other men who have sex with men’s views of more inclusive criteria for source plasma donation. BMC Public Health, 23, 768. https://doi.org/10.1186/s12889-023-15424-1
- Goldman, M., Butler-Foster, T., Lapierre, D., O'Brien, S. F., & Devor, A. (2020). Trans people and blood donation. Transfusion.
- Haw, J., Butler-Foster, T., Murray, B., Lapierre, D., Bosse, J., Edwards, J., Gümüşpala, Ş., Jenkins, C., & Devor, A. (2024). Advancing gender inclusivity for Two-Spirit, trans, nonbinary and other gender-diverse blood and plasma donors. Vox Sang, 119(5), 409-416. https://doi.org/10.1111/vox.13596
- Haw, J., Walrond, J., Jayachandran, J., Dordunoo, D., Eche-Ameh, H., Muwhen, U., Phiri, P., Rastogi, J., & Tinga, B. (2023). Sickle cell disease and the need for blood: Barriers to donation for African, Caribbean, and Black young adults in Canada. Transfusion, 63(7), 1324-1332. https://doi.org/10.1111/trf.17396
- Tran, N. Y., Charbonneau, J., & Valderrama-Benitez, V. (2013). Blood donation practices, motivations and beliefs in Montreal's Black communities: the modern gift under a new light. Ethn Health, 18(6), 508-529. https://doi.org/10.1080/13557858.2012.734279
- Holloway, K. (2023). Exploring the increasing need for plasma collection: Perspectives of voluntary nonremunerated donors on payment for plasma in Canada. Transfus Med., 33(5), 390-397. https://doi.org/10.1111/tme.12992
- France, C. R., France, J. L., & Himawan, L. K. (2022). What would it take to convince you to donate? A survey study of the relationship between motivators, barriers, and payment for whole blood, plasma, and platelet donation. Transfusion, 62(6), 1251-1260. https://doi.org/10.1111/trf.16886
- Holloway, K. (2022). Understanding the experiences of plasma donors in Canada's new source plasma collection centres during COVID-19: A qualitative study. Vox Sang, 1078-1084. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9348189
- Holloway, K. (2023). Emotional Labor of Nurses and Phlebotomists in a New Source Plasma Collection Site During the COVID-19 Pandemic. Global qualitative nursing research, 10, 23333936231192000. https://doi.org/10.1177/23333936231192000
- Vesnaver, E., Gibson, E., Goldman, M., Butler‐Foster, T., Hill, N. E., Lapierre, D., MacDonagh, R., Rubini, K. A., Miguel, G., Rosser, A., MacPherson, P., Palumbo, A., Randall, T., Osbourne‐Sorrell, W., O'Brien, S. F., Otis, J., Greaves, M., Al‐Bakri, T. B., Reid, M., . . . Presseau, J. (2023). Navigating imperfect policies to donate plasma: Survey on plasma donation and a pilot plasma donation program among men who have sex with men in Canada. Transfusion (Philadelphia, Pa.), 63(6), 1172-1183. https://doi.org/10.1111/trf.17398
- Butler-Foster, T., Chin-Yee, I., Huang, M., & Jackson, K. T. (2020). Toward Understanding Culturally Sensitive Care for Transgender Blood Donors: A Scoping Review of Health Care Provider Knowledge. Transgender Health, 5(2), 104-115. https://doi.org/10.1089/trgh.2019.0062
- Makin, J. K., Francis, K., Polonsky, M., & Renzaho, A. M. N. (2019). Interventions to increase blood donation among ethnic/racial minorities: a systematic review. https://doi.org/10.1155/2019/6810959
- Tran, N. Y. L., Charbonneau, J., & Valderrama-Benitez, V. (2013). Blood donation practices, motivations and beliefs in Montreal's Black communities: the modern gift under a new light. Ethnicity & Health, 18(6), 508-529. https://doi.org/10.1080/13557858.2012.734279
- Muñoz-Bravo, C., Gutiérrez-Bedmar, M., Gómez-Aracena, J., García-Rodríguez, A., & Navajas, J. F. (2013). Iron: protector or risk factor for cardiovascular disease? Still controversial. Nutrients, 5(7), 2384-2404. https://doi.org/10.3390/nu5072384
- Quee, F. A., Peffer, K., Ter Braake, A. D., & Van den Hurk, K. (2022). Cardiovascular Benefits for Blood Donors? A Systematic Review. Transfus Med Rev, 36(3), 143-151. https://doi.org/10.1016/j.tmrv.2022.04.004
- Canadian Blood Services. (2024). Eligibility: hemoglobin and iron. Canadian Blood Services. Retrieved September 16, 2025 from https://www.blood.ca/en/blood/am-i-eligible-donate-blood/eligibility/hemoglobin-iron
- Assi, T. B., & Baz, E. (2014). Current applications of therapeutic phlebotomy. Blood Transfus, 12 Suppl 1(Suppl 1), s75-s83. https://doi.org/10.2450/2013.0299-12
- Rosa-Bray, M., Wisdom, C., Marier, J. F., Mouksassi, M. S., & Wada, S. (2015). The effect of plasmapheresis on blood pressure in voluntary plasma donors. Vox Sang, 108(1), 11-17. https://doi.org/10.1111/vox.12188
- Rosa-Bray, M., Wisdom, C., Wada, S., Johnson, B. R., Grifols-Roura, V., & Grifols-Lucas, V. (2013). Prospective multicentre study of the effect of voluntary plasmapheresis on plasma cholesterol levels in donors. Vox Sang, 105(2), 108-115. https://doi.org/10.1111/vox.12031
- Ferguson, E., Taylor, M., Keatley, D., Flynn, N., & Lawrence, C. (2012). Blood donors' helping behavior is driven by warm glow: more evidence for the blood donor benevolence hypothesis. Transfusion, 52(10), 2189-2200. https://doi.org/10.1111/j.1537-2995.2011.03557.x
- Mikkelsen, C., Mori, G., van Walraven, S. M., Castrén, J., Zahra, S., MacLennan, S., Seidel, K., Fontana, S., Veropalumbo, E., Cannata, L., Pupella, S., Kvist, M., Happel, M., Korkalainen, P., Wulff, B., Fernandez-Sojo, J., Eguizabal, C., Urbano, F., Vesga, M. A., . . . Ullum, H. (2021). Putting the spotlight on donation-related risks and donor safety - are we succeeding in protecting donors? Vox Sang, 116(3), 313-323. https://doi.org/10.1111/vox.13014
- Radovčić, M. K., Ljubičić, J., Očić, T., Jukić, I., & Vuk, T. (2021). Blood collection failures from a blood establishment perspective. Transfus Med, 31(2), 88-93. https://doi.org/10.1111/tme.12762
- Young, P., Crowder, L., Steele, W., Irving, D., Pink, J., Kutner, J. M., Yokoyama, A. P. H., Van Buren, N., O'Sullivan, N. W., Sayers, M., Alcantara, R. M., van den Hurk, K., Wiersum-Osselton, J., & Shaz, B. (2021). Frequency of rare, serious donor reactions: International perspective. Transfusion, 61(6), 1780-1788. https://doi.org/10.1111/trf.16333
- Thijsen, A., & Masser, B. (2019). Vasovagal reactions in blood donors: risks, prevention and management. Transfus Med, 29 Suppl 1, 13-22. https://doi.org/10.1111/tme.12488
- Goldman, M., Land, K., Robillard, P., & Wiersum-Osselton, J. (2016). Development of standard definitions for surveillance of complications related to blood donation. Vox Sang, 110(2), 185-188. https://doi.org/10.1111/vox.12323
- Takanashi, M., Odajima, T., Aota, S., Sudoh, M., Yamaga, Y., Ono, Y., Yoshinaga, K., Motoji, T., Matsuzaki, K., Satake, M., Sugimori, H., & Nakajima, K. (2012). Risk factor analysis of vasovagal reaction from blood donation. Transfusion and Apheresis Science, 47(3), 319-325. https://doi.org/10.1016/j.transci.2012.04.002
- Donald, S. J., McIntyre, W. F., Dingwall, O., Hiebert, B., Ponnampalam, A., & Seifer, C. M. (2019). Is donating blood for the faint of heart? a systematic review of predictors of syncope in whole blood donors. Transfusion, 59(9), 2865-2869. https://doi.org/10.1111/trf.15442
- Thijsen, A., Masser, B., Davison, T. E., van Dongen, A., & Williams, L. A. (2023). Beyond fear: A longitudinal investigation of emotions and risk of a vasovagal reaction in first-time whole-blood donors. Transfusion, 63(1), 163-170. https://doi.org/10.1111/trf.17169
- Gilchrist, P. T., Thijsen, A., Masser, B. M., France, C. R., & Davison, T. E. (2021). Improving the donation experience and reducing venipuncture pain by addressing fears among whole-blood and plasma donors. Transfusion, 61(7), 2107-2115. https://doi.org/10.1111/trf.16407
- Lewin, A., Deschênes, J., Rabusseau, I., Thibeault, C., Renaud, C., & Germain, M. (2023). Pre-donation water and salty snacks to prevent vasovagal reactions among blood donors. Transfusion, 63(1), 156-162. https://doi.org/10.1111/trf.17173
- Van Remoortel, H., Van de Sande, D., Maes, D., Khoudary, J., Tavernier, V., Tiberghien, P., De Buck, E., & Compernolle, V. (2024). The efficacy and effectiveness of drinking interventions to reduce vasovagal reactions in blood donors: A systematic review and meta-analysis. Vox Sang, 119(11), 1129-1140. https://doi.org/10.1111/vox.13724
- Wu, Y., Qi, H., Di Angelantonio, E., Kaptoge, S., Wood, A. M., & Kim, L. G. (2025). Risk factors for vasovagal reactions in blood donors: A systematic review and meta-analysis. Transfusion, 65(1), 211-223. https://doi.org/10.1111/trf.18078
- Newman, B. H., & Waxman, D. A. (1996). Blood donation-related neurologic needle injury: evaluation of 2 years' worth of data from a large blood center. Transfusion, 36(3), 213-215. https://doi.org/10.1046/j.1537-2995.1996.36396182137.x
- Nocera, G., & Jacob, C. (2020). Mechanisms of Schwann cell plasticity involved in peripheral nerve repair after injury. Cell Mol Life Sci, 77(20), 3977-3989. https://doi.org/10.1007/s00018-020-03516-9
- Brittenham, G. M. (2011). Iron deficiency in whole blood donors. Transfusion (Philadelphia, Pa.), 51(3), 458-461. https://doi.org/10.1111/j.1537-2995.2011.03062.x
- Popovsky, M. A. (2012). Anemia, iron depletion, and the blood donor: it's time to work on the donor's behalf. Transfusion (Philadelphia, Pa.), 52(4), 688-692. https://doi.org/10.1111/j.1537-2995.2012.03562.x
- Association for the Advancement of Blood and Biotherapies (AABB). (2017). Updated strategies to limit or prevent iron deficiency in blood donors. Revised July 2022 (Bulletin #17-02, Issue. https://www.aabb.org/docs/default-source/default-document-library/resources/association-bulletins/ab19-02-revised.pdf?sfvrsn=a176ae2c_4
- Mantadakis, E., Panagopoulou, P., Kontekaki, E., Bezirgiannidou, Z., & Martinis, G. (2022). Iron Deficiency and Blood Donation: Links, Risks and Management. J Blood Med, 13, 775-786. https://doi.org/10.2147/jbm.S375945
- Kiss, J. E., Brambilla, D., Glynn, S. A., Mast, A. E., Spencer, B. R., Stone, M., Kleinman, S. H., & Cable, R. G. (2015). Oral Iron Supplementation After Blood Donation: A Randomized Clinical Trial. JAMA : the journal of the American Medical Association, 313(6), 575-583. https://doi.org/10.1001/jama.2015.119
- Cable, R. G., Glynn, S. A., Kiss, J. E., Mast, A. E., Steele, W. R., Murphy, E. L., Wright, D. J., Sacher, R. A., Gottschall, J. L., Tobler, L. H., & Simon, T. L. (2012). Iron deficiency in blood donors: the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion, 52(4), 702-711. https://doi.org/10.1111/j.1537-2995.2011.03401.x
- Goldman, M., Uzicanin, S., Scalia, V., & O'Brien, S. F. (2014). Iron deficiency in Canadian blood donors. Transfusion, 54(3 Pt 2), 775-779. https://doi.org/10.1111/trf.12380
- Newman, B. (2006). Iron depletion by whole-blood donation harms menstruating females: the current whole-blood-collection paradigm needs to be changed. Transfusion, 46(10), 1667-1681. https://doi.org/10.1111/j.1537-2995.2006.00969.x
- Goldman, M., Uzicanin, S., Osmond, L., Scalia, V., & O'Brien, S. F. (2017). A large national study of ferritin testing in Canadian blood donors. Transfusion, 57(3), 564-570. https://doi.org/10.1111/trf.13956
- Goldman, M., Uzicanin, S., Scalia, J., Scalia, V., & O'Brien, S. F. (2016). Impact of informing donors of low ferritin results. Transfusion, 56(9), 2193-2198. https://doi.org/10.1111/trf.13691
- Baart, A. M., van Noord, P. A., Vergouwe, Y., Moons, K. G., Swinkels, D. W., Wiegerinck, E. T., de Kort, W. L., & Atsma, F. (2013). High prevalence of subclinical iron deficiency in whole blood donors not deferred for low hemoglobin. Transfusion, 53(8), 1670-1677. https://doi.org/10.1111/j.1537-2995.2012.03956.x
- Rigas, A. S., Sørensen, C. J., Pedersen, O. B., Petersen, M. S., Thørner, L. W., Kotzé, S., Sørensen, E., Magnussen, K., Rostgaard, K., Erikstrup, C., & Ullum, H. (2014). Predictors of iron levels in 14,737 Danish blood donors: results from the Danish Blood Donor Study. Transfusion, 54(3pt2), 789-796. https://doi.org/10.1111/trf.12518
- Salvin, H. E., Pasricha, S. R., Marks, D. C., & Speedy, J. (2014). Iron deficiency in blood donors: a national cross-sectional study. Transfusion, 54(10), 2434-2444. https://doi.org/10.1111/trf.12647
- Meulenbeld, A., Ramondt, S., Sweegers, M. G., Quee, F. A., Prinsze, F. J., Hoogendijk, E. O., Swinkels, D. W., & van den Hurk, K. (2024). Effectiveness of ferritin-guided donation intervals in whole-blood donors in the Netherlands (FIND'EM): a stepped-wedge cluster-randomised trial. Lancet, 404(10447), 31-43. https://doi.org/10.1016/s0140-6736(24)01085-7
- Cable, R. G., Birch, R. J., Spencer, B. R., Wright, D. J., Bialkowski, W., Kiss, J. E., Rios, J., Bryant, B. J., & Mast, A. E. (2017). The operational implications of donor behaviors following enrollment in STRIDE (Strategies to Reduce Iron Deficiency in blood donors). Transfusion, 57(10), 2440-2448. https://doi.org/10.1111/trf.14226
- Pasricha, S.-R., McQuilten, Z. K., Keller, A. J., & Wood, E. M. (2011). Hemoglobin and iron indices in nonanemic premenopausal blood donors predict future deferral from whole blood donation. Transfusion, 51(12), 2709-2713. https://doi.org/10.1111/j.1537-2995.2011.03173.x
- Benson, C. S., Shah, A., Stanworth, S. J., Frise, C. J., Spiby, H., Lax, S. J., Murray, J., & Klein, A. A. (2021). The effect of iron deficiency and anaemia on women's health. Anaesthesia, 76 Suppl 4, 84-95. https://doi.org/10.1111/anae.15405
- Pratt, J. J., & Khan, K. S. (2016). Non-anaemic iron deficiency - a disease looking for recognition of diagnosis: a systematic review. Eur J Haematol, 96(6), 618-628. https://doi.org/10.1111/ejh.12645
- Houston, B. L., Hurrie, D., Graham, J., Perija, B., Rimmer, E., Rabbani, R., Bernstein, C. N., Turgeon, A. F., Fergusson, D. A., Houston, D. S., Abou-Setta, A. M., & Zarychanski, R. (2018). Efficacy of iron supplementation on fatigue and physical capacity in non-anaemic iron-deficient adults: a systematic review of randomised controlled trials. BMJ Open, 8(4), e019240. https://doi.org/10.1136/bmjopen-2017-019240
- Petraglia, F., & Dolmans, M. M. (2022). Iron deficiency anemia: Impact on women's reproductive health. Fertil Steril, 118(4), 605-606. https://doi.org/10.1016/j.fertnstert.2022.08.850
- Camaschella, C. (2015). Iron deficiency: new insights into diagnosis and treatment. Hematology Am Soc Hematol Educ Program, 2015, 8-13. https://doi.org/10.1182/asheducation-2015.1.8
- Munro, M. G., Mast, A. E., Powers, J. M., Kouides, P. A., O'Brien, S. H., Richards, T., Lavin, M., & Levy, B. S. (2023). The relationship between heavy menstrual bleeding, iron deficiency, and iron deficiency anemia. Am J Obstet Gynecol, 229(1), 1-9. https://doi.org/10.1016/j.ajog.2023.01.017
- Beard, J. L., Dawson, H., & Piñero, D. J. (1996). Iron metabolism: a comprehensive review. Nutr Rev, 54(10), 295-317. https://doi.org/10.1111/j.1753-4887.1996.tb03794.x
- Falkingham, M., Abdelhamid, A., Curtis, P., Fairweather-Tait, S., Dye, L., & Hooper, L. (2010). The effects of oral iron supplementation on cognition in older children and adults: a systematic review and meta-analysis. Nutr J, 9, 4. https://doi.org/10.1186/1475-2891-9-4
- Bryant, B. J., Yau, Y. Y., Arceo, S. M., Hopkins, J. A., & Leitman, S. F. (2013). Ascertainment of iron deficiency and depletion in blood donors through screening questions for pica and restless legs syndrome. Transfusion, 53(8), 1637-1644. https://doi.org/10.1111/trf.12061
- Cable, R. G., Brambilla, D., Glynn, S. A., Kleinman, S., Mast, A. E., Spencer, B. R., Stone, M., & Kiss, J. E. (2016). Effect of iron supplementation on iron stores and total body iron after whole blood donation. Transfusion, 56(8), 2005-2012. https://doi.org/10.1111/trf.13659
- Krayenbuehl, P. A., Battegay, E., Breymann, C., Furrer, J., & Schulthess, G. (2011). Intravenous iron for the treatment of fatigue in nonanemic, premenopausal women with low serum ferritin concentration. Blood, 118(12), 3222-3227. https://doi.org/10.1182/blood-2011-04-346304
- Snook, J., Bhala, N., Beales, I. L. P., Cannings, D., Kightley, C., Logan, R. P., Pritchard, D. M., Sidhu, R., Surgenor, S., Thomas, W., Verma, A. M., & Goddard, A. F. (2021). British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut, 70(11), 2030-2051. https://doi.org/10.1136/gutjnl-2021-325210
- Hoad, V. C., Castrén, J., Norda, R., & Pink, J. (2024). A donor safety evidence literature review of the short- and long-term effects of plasmapheresis. Vox Sang, 119(2), 94-101. https://doi.org/10.1111/vox.13512
- European Directorate for the Quality of Medicines & HealthCare of the Council of Europe (EDQM). (2023). The Guide to the preparation, use and quality assurance of blood components, 21st Edition,. In. Strasbourg, France.
- Buzza, M., Marks, D. C., Capper, H., Cassin, E., Badcock, C. A., Reid, S., Kwok, M., Yang, H., Lee, J., Corrigan, C., Hartkopf-Theis, T., & Keller, A. (2012). A prospective trial assessing the safety and efficacy of collecting up to 840 mL of plasma in conjunction with saline infusion during plasmapheresis. Transfusion, 52(8), 1806-1813. https://doi.org/10.1111/j.1537-2995.2012.03561.x
- Evers, J., Schreiber, G. B., & Taborski, U. (2022). Impact of saline infusion and citrate infusion rate during donor plasmapheresis. J Clin Apher, 37(6), 584-591. https://doi.org/10.1002/jca.22025
- Vassallo, R. R., Bravo, M. D., & Kamel, H. (2017). Improved donor safety in high-volume apheresis collections. Transfusion, 57(2), 319-324. https://doi.org/10.1111/trf.13897
- Lee, G., & Arepally, G. M. (2012). Anticoagulation techniques in apheresis: from heparin to citrate and beyond. J Clin Apher, 27(3), 117-125. https://doi.org/10.1002/jca.21222
- Bialkowski, W., Bruhn, R., Edgren, G., & Papanek, P. (2016). Citrate anticoagulation: Are blood donors donating bone? J Clin Apher, 31(5), 459-463. https://doi.org/10.1002/jca.21438
- Winters, J. L. (2006). Complications of donor apheresis. J Clin Apher, 21(2), 132-141. https://doi.org/10.1002/jca.20039
- Leitman, S. F., Boltansky, H., Alter, H. J., Pearson, F. C., & Kaliner, M. A. (1986). Allergic reactions in healthy plateletpheresis donors caused by sensitization to ethylene oxide gas. N Engl J Med, 315(19), 1192-1196. https://doi.org/10.1056/nejm198611063151904
- Leitman, S. F., Boltansky, H., Alter, H. J., Pearson, F. C., & Kaliner, M. A. (1986). Allergic Reactions in Healthy Platelet-Pheresis Donors Caused by Sensitization to Ethylene Oxide Gas. New England Journal of Medicine, 315(19), 1192-1196. https://doi.org/10.1056/nejm198611063151904
- Centers for Disease Control and Prevention (CDC). (2023, November 28, 2023). Ethylene Oxide "Gas" Sterilzation. Retrieved October 2, 2024 from https://www.cdc.gov/infection-control/hcp/disinfection-sterilization/ethylene-oxide-sterilization.html
- Working Group on Donor Vigilance of the International Society of Blood Transfusion of the Working Party on Haemovigilance (ISBT), The International Haemovigilance Network (IHN), & The AABB Donor Haemovigilance Working Group. (2014). Standard for Surveillance of Complications Related to Blood Donation. In: Association for the Advancement of Blood and Biotherapies (AABB).
- Gansner, J. M., Rahmani, M., Jonsson, A. H., Fortin, B. M., Brimah, I., Ellis, M., Smeland-Wagman, R., Li, Z. J., Schenkel, J. M., Brenner, M. B., Yefidoff-Freedman, R., Sloan, S. R., Berliner, N., Issa, N. C., Baden, L. R., Longo, D. L., Wesemann, D. R., Neuberg, D., Rao, D. A., & Kaufman, R. M. (2019). Plateletpheresis-associated lymphopenia in frequent platelet donors. Blood, 133(6), 605-614. https://doi.org/10.1182/blood-2018-09-873125
- Rahmani, M., Fortin, B. M., Berliner, N., Issa, N., Neuberg, D., Kaufman, R. M., & Gansner, J. M. (2019). CD4+ T-cell lymphopenia in frequent platelet donors who have ceased platelet donation for at least 1 year. Transfusion, 59(5), 1644-1647. https://doi.org/10.1111/trf.15192
- Shanbrom, E., Lundak, R., & Walford, R. L. (1972). Long-term Plasmapheresis: Effects on Specific Plasma Proteins. Transfusion, 12(3), 162-167. https://doi.org/10.1111/j.1537-2995.1972.tb00003.x
- Simon, T., Kutvirt, S., & Levis, S. (1989). Immune changes after long-term apheresis donations. 31st Annual Meeeting of the American Hematology Society, Atlanta.
- Kliman, A., P. Carbone, P., Gaydos, L. A., & Freireich, E. J. (1964). Effects of Intensive Plasmapheresis on Normal Blood Donors. Blood, 23(5), 647-656. https://doi.org/10.1182/blood.V23.5.647.647
- Wasi, S., Santowski, T., Murray, S. A., Perrault, R. A., & Gill, P. (1991). The Canadian Red Cross Plasmapheresis Donor Safety Program: Changes in Plasma Proteins after Long-Term Plasmapheresis. Vox Sang, 60(2), 82-87. https://doi.org/10.1111/j.1423-0410.1991.tb00879.x
- Ciszewski, T. S., Ralston, S., Acteson, D., Wasi, S., & Strong, S. J. (1993). Protein levels and plasmapheresis intensity. Transfus Med, 3(1), 59-65. https://doi.org/10.1111/j.1365-3148.1993.tb00105.x
- Bechtloff, S., Tran-My, B., Haubelt, H., Stelzer, G., Anders, C., & Hellstern, P. (2005). A prospective trial on the safety of long-term intensive plasmapheresis in donors. Vox Sang, 88(3), 189-195. https://doi.org/10.1111/j.1423-0410.2005.00632.x
- Tran-Mi, B., Storch, H., Seidel, K., Schulzki, T., Haubelt, H., Anders, C., Nagel, D., Siegler, K. E., Vogt, A., Seiler, D., & Hellstern, P. (2004). The impact of different intensities of regular donor plasmapheresis on humoral and cellular immunity, red cell and iron metabolism, and cardiovascular risk markers. Vox Sang, 86(3), 189-197. https://doi.org/10.1111/j.0042-9007.2004.00408.x
- Bialkowski, W., Blank, R. D., Zheng, C., Gottschall, J. L., & Papanek, P. E. (2019). Impact of frequent apheresis blood donation on bone density: A prospective, longitudinal, randomized, controlled trial. Bone Rep, 10, 100188. https://doi.org/10.1016/j.bonr.2018.100188
- Grau, K., Vasan, S. K., Rostgaard, K., Bialkowski, W., Norda, R., Hjalgrim, H., & Edgren, G. (2017). No association between frequent apheresis donation and risk of fractures: a retrospective cohort analysis from Sweden. Transfusion, 57(2), 390-396. https://doi.org/10.1111/trf.13907