Professional Education
Learn.Share.Advance
Surveillance Report 2020
We are pleased to present this annual report describing transmissible blood-borne infection surveillance. High quality and timely surveillance is central to the safety of the blood supply. This includes monitoring of transmissible disease markers that the blood is tested for (including bacteria) and investigation of any reports of possible transfusion transmission, as well as a horizon scan for any new pathogens that may pose a risk.
To request older Surveillance Reports, please contact us through the Feedback form.
Current issue - 2023
Surveillance Report 2020
Author: Sheila O'Brien, RN, PhD
Online publication date: August 2021
Executive summary
This annual report describes surveillance of transmissible blood-borne infections and emerging threats of concern. High quality and timely surveillance is central to the safety of the blood supply. This includes monitoring of transmissible disease markers that the blood is tested for and investigation of any reports of possible transfusion transmission, as well as a horizon scan for any new pathogens that may pose a risk. Non-infectious surveillance of aspects of donor health and safety as well as diagnostic services are also included.
Infectious risk monitoring
The most up-to-date tests for pathogens are used to identify infectious donations and prevent their release for patient use. In 2020, transmissible disease rates per 100,000 donations continued to be very low: 0 HIV, hepatitis C (HCV) 5.0, hepatitis B (HBV) 5.0, HTLV 0.9 and syphilis 9.8. Selective testing of donors at risk of Chagas disease identified no positive donations, and there were 12 donations positive for West Nile Virus (WNV). Residual risk estimates of a potentially infectious donation from a unit of blood are very low at 1 in 12.9 million donations for HIV, 1 in 27.1 million donations for HCV and 1 in 2.0 million donations for HBV. Lookback and traceback investigations did not identify any transfusion transmitted infections. Bacterial growth was identified in 175 platelet products. Of 114 potential peripheral stem cell or bone marrow donors tested, none were positive for any transmissible infection markers. Of 283 samples from mothers donating stem cells collected from the umbilical cord and placenta (called “cord blood”) after their babies were born, none were positive for any marker.
Horizon scanning for emerging pathogens monitors potential threats to safety. Risk of a tick- borne disease, babesiosis, continues to be monitored. The parasite (Babesia microti) that causes babesiosis appears to be in the early stages of becoming established in a few places in Canada, especially in Manitoba. Travelers and former residents from malaria risk areas are temporarily deferred for malaria risk. In addition, a 3 week deferral for any travel outside Canada, the USA and Europe reduces risk from short term travel related infections, such as Zika virus. This was extended to include any travel outside of Canada in 2020 to reduce risk of exposure to COVID-19 to other donors and staff.
COVID-19
A novel coronavirus (SARS-CoV-2) was identified in Wuhan, Hubei Province, China in November 2019. On March 11th, 2020 the World Health Organization declared a COVID-19 pandemic. SARS-CoV-2 is not transmissible by blood but to keep donors, volunteers and staff safe numerous changes were made in the blood collections environment. Canadian Blood Services has tested over 100,000 blood samples since May for SARS-CoV-2 antibodies in collaboration with the COVID-19 Immunity Task Force commissioned by the Canadian Federal Government. Seroprevalence has been low (less than 2% of donors) showing most people were susceptible to SARS-CoV-2 infection. This information was very important for Public Health officials to plan safety interventions for Canadians. In 2021 this study will monitor antibody response to vaccine roll-out and natural infections.
Canadian Blood Services needed to quickly put in place measures to reduce risk to donors, volunteers and staff, and to ensure adequacy of the blood supply. Giving blood is very safe, and serious reactions in donors are quite rare. A Donor Wellness initiative was implemented in March 2019 which reduced vasovagal (feeling faint) reactions and helped donors to feel well after donating. To reduce points of contact that may be a risk for COVID-19 transmission, these were modified with no increase in the vasovagal reaction rate. Deferrals for travel, having COVID-19 or contact with someone with COVID-19 were started, but few donors were deferred (<0.2%). To reduce deferrals and ensure adequacy of the blood supply if donor attendance dropped during the pandemic from July to October the minimum hemoglobin required to donate was reduced from 125 g/L to 120 g/L for women and from 130 g/L to 125 g/L for men. The deferrals decreased from 7% to 3.2% for females and from 1.5% to 0.8% for males during that period.
Diagnostic services laboratories
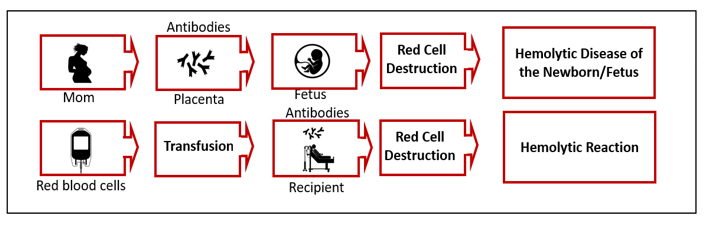
The Diagnostic Services Laboratories at Canadian Blood Services provide prenatal testing for some pregnant women, including all pregnancies in several provinces, and for some patients with complex transfusion needs. In 2020 1,160 red blood cell antibodies were identified in pregnant women that may pose a risk of hemolytic disease of the fetus/newborn and 1,430 red cell antibodies were identified in patients who may need special matching for transfusion.
1. Introduction
Safety of the blood supply from pathogens involves a multifaceted approach. Donor education materials on the internet and required reading just before donating explain risk factors for transmissible infections and who should not donate. Before donating blood, everyone must complete a health history questionnaire which includes questions about specific risk factors for transmissible infections. This is followed by an interview with trained staff to decide if the person is eligible to donate blood. All donations are tested for markers of transfusion transmissible agents including HIV, HBV, HCV, human T-cell lymphotropic virus (HTLV) (a rare cause of leukemia) and syphilis. WNV testing is done during the at-risk period of the year (spring, summer and fall) and in at-risk travelers during the winter. In addition, donors at risk of Chagas disease (which is transmitted by the bite of an insect in Latin America) are tested, and all platelet products are tested for bacteria. A new coronavirus, SARS-CoV-2, which causes the respiratory infection, COVID-19, emerged in 2020 but it is not transmitted by blood transfusion. However, there was an impact on operational issues to ensure safety for donors, staff and volunteers while meeting the needs of blood recipients. Additionally, epidemiologic data on the frequency of antibodies in our donor population over time provided support for public health decision making during the pandemic.
Surveillance includes monitoring of transmissible infection testing in donors, investigation of possible transfusion transmitted infections in recipients and horizon scanning for new, emerging pathogens. Monitoring the safety of donors is also essential. Although surveillance is conducted in "real time" over each year, final verification steps generally impose a short delay in producing a final report. Surveillance also includes monitoring of donor safety. This report describes Canadian Blood Services’ approach to surveillance of transmissible blood-borne infection, infectious threats and donor safety, as well as data for the calendar year of 2020.
2. Blood donor surveillance
The numbers of allogeneic blood donations (whole blood and platelet and plasma apheresis) from first time and repeat donors are shown in Figure 1. The majority of donations are from repeat donors (90.2%) with 9.8% of donations from new donors. The decrease in blood collections in 2020 was at least partially due to surgery cancellations related to SARS-CoV-2.
Image
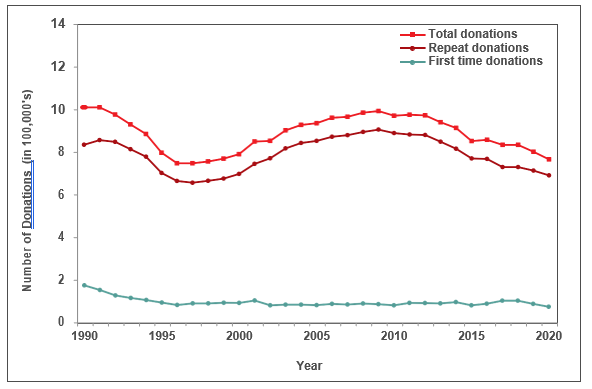
FIgure 1: Donations in all Canadian Blood Services Regions, 1990-2020
Note: Source plasma donations are not included.
The “Classical” pathogens
Details of screening tests used, and dates of implementation are shown in Appendix 1. In Table 1 the numbers of positive donations and the rates of positive tests per 100,000 donations are shown for 2020 by demographic groups. When a transmissible infection is detected, it is most often in a first-time donor as these donors have not been tested previously and may have acquired the infection at any time in their lives. All transmissible infection positive donations occurred in whole blood donations except one HBV positive apheresis donation. There were no HIV positive donations in 2020. In the past 5 years the number of HIV positive donations has ranged from 1 to 4 per year. The rate per 100,000 donations has decreased for most markers and the rate for repeat donations is extremely low (see Appendix 2). The exception is syphilis which has increased in 2020 from 4.1 per 100,000 donations in 2019 to 9.8 in 2020, with the increase tending to be greater in repeat donors rather than first-time donors. Syphilis cases have also been increasing in the general population but are not directly comparable because public health cases only include people who had reason to be tested (usually new infections with symptoms) whereas blood donors include both people unaware of their infection and those who may have been infected in the past. It is unlikely that syphilis could be transmitted by transfusion due to modern blood processing methods.
Table 1: Confirmed positive donations and prevalence rates per 100,000 donations in 2020
| Characteristic | Number of Donations | Percent of Donations | HIV | HCV | HBV | HTLV | Syphilis | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pos | Rate | Pos | Rate | Pos | Rate | Pos | Rate | Pos | Rate | |||
| Donor status | ||||||||||||
|
First time |
75,293 | 9.8 | 0 | - | 36 | 47.8 | 35 | 46.5 | 5 | 6.6 | 41 | 54.5 |
|
Repeat |
690,516 | 90.2 | 0 | - | 2 | 0.3 | 3 | 0.4 | 2 | 0.3 | 34 | 4.9 |
| Sex | ||||||||||||
|
Female |
341,997 | 44.7 | 0 | - | 23 | 6.7 | 7 | 2.1 | 7 | 2.1 | 17 | 5.0 |
|
Male |
423,812 | 55.3 | 0 | - | 15 | 3.5 | 31 | 7.3 | 0 | - | 58 | 13.7 |
| Age | ||||||||||||
|
17-29 |
149,879 | 19.6 | 0 | - | 3 | 2.0 | 7 | 4.7 | 0 | - | 17 | 11.3 |
|
30-39 |
143,334 | 18.7 | 0 | - | 8 | 5.6 | 13 | 9.1 | 1 | 0.7 | 21 | 14.7 |
|
40-49 |
126,671 | 16.5 | 0 | - | 8 | 6.3 | 9 | 7.1 | 4 | 3.2 | 15 | 11.8 |
|
50+ |
345,925 | 45.2 | 0 | - | 19 | 5.5 | 9 | 2.6 | 2 | 0.6 | 22 | 6.4 |
| Total | 765,809 | 100 | 0 | - | 38 | 5.0 | 38 | 5.0 | 7 | 0.9 | 75 | 9.8 |
All transmissible infection positive donations are destroyed. The main source of risk is when a blood donor acquired the infection too recently to be detected by testing. This is called the “window period” of infection. With current testing the window period is very short. For HIV and HCV an infection would be detected within 1 to 2 weeks of a donor being infected by nucleic acid testing (NAT) and for HBV within one month. The residual risk of infection is the estimated risk of a potentially infectious donation being given during the “window period”. These estimates, shown in Table 2 are based on new infections (positive donations with a prior donation which tested negative within the last 3 years) and include 2018 -2020 data. The risk is currently extremely low, but of course it can never be zero.
Table 2: Estimated residual risk of HIV, HCV and HBV
| HIV | HCV | HBV |
|---|---|---|
| 1 in 12.9 million donations | 1 in 27.1 million donations | 1 in 2.0 million donations |
Risk factors
Risk factor interviews are carried out with donors who test positive for transmissible infections. The main risk factors are shown in Table 3. HIV infections are very rare in donors; therefore it is difficult to generalize the risk factors. It should be noted that participation is voluntary and therefore there are only data for some donors, and that for many donors no risk factors were identified.
Table 3: Risk factors for infectious disease in blood donors
| Infection | Risk Factor |
|---|---|
| HIV | High risk heterosexual partners Male to male sex |
| HCV |
History of intravenous drug use Born in Africa or Asia |
| HBV | Born in Africa or Asia |
| HTLV | Born overseas (especially Caribbean) History of other sexually transmitted disease History of blood transfusion |
| Syphilis | Previous history of syphilis |
Note: Not all donors are interviewed
Chagas disease (Trypanosoma cruzi)
Chagas disease is caused by infection with a parasite called Trypanosoma cruzi (T. cruzi). People can become infected with it after being bitten by an insect found in parts of Mexico, Central and South America. The T. cruzi parasite can also be passed on from mother to child during pregnancy and by blood transfusion. Since Canadian Blood Services implemented testing of at-risk donors in 2010, 35 T. cruzi positive donations have been identified (see Figure 2). There were no positive donations in 2020 of 9,201 tested.
Image
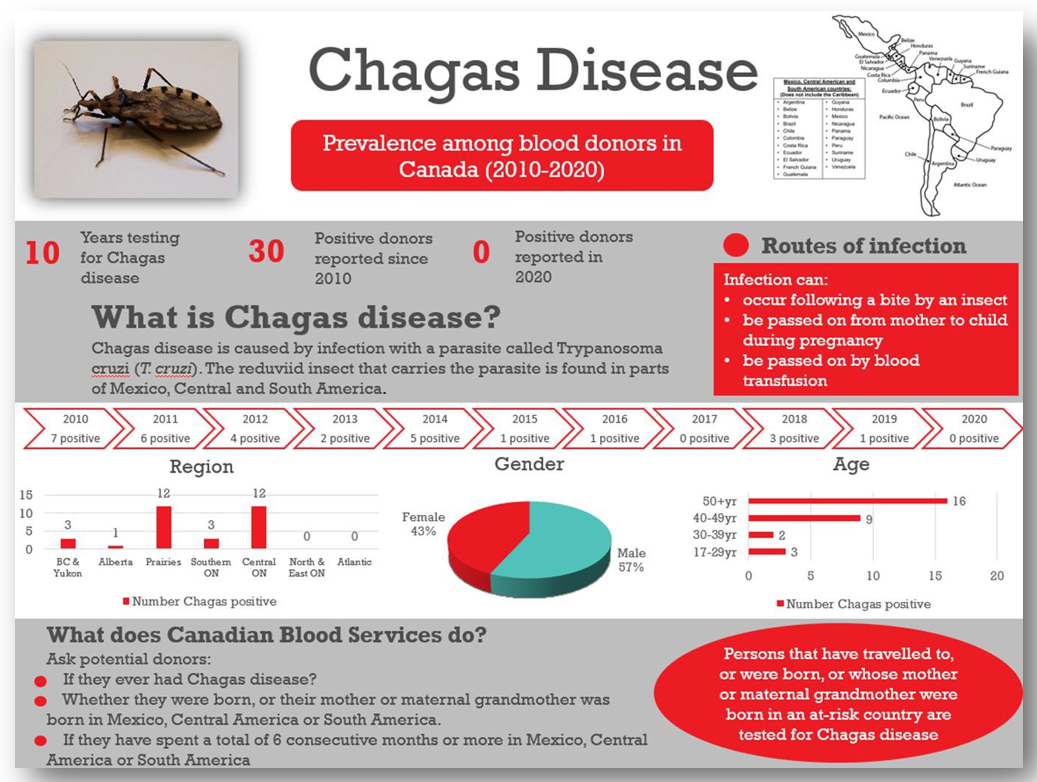
Figure 2: Chagas Disease testing results 2010 to 2020
West Nile virus
West Nile virus is a mosquito-borne virus that has been present in North America since 1999 (in Canada since 2002). Although symptoms can be severe, they are usually mild, and most people are not aware of their infection. During spring, summer and fall, donations are routinely tested in mini-pools of 6 donations. However, to further reduce the risk, an algorithm is applied to identify all donations from areas where West Nile virus is active, and these are tested as single donations. In 2020, 394,834 donations were tested over the spring/summer/fall when all donations were tested, and 12 donations were positive, identified from August 4 to September 7. All positive donations were from Ontario corresponding with the location of clinical cases. With only travelers tested over the winter, 35,533 donations (from Jan 1 to May 31, 2020 and November 29 to December 31, 2020) were tested and none found to be positive.
Image
3. Surveillance for emerging pathogens
A horizon scan of potential blood borne infections in the general community ensures rapid revision of donor policies to maintain safety. Even before a new infectious disease is reported in Canada, we are aware of emerging infectious agents by monitoring outbreaks in other parts of the world. International travel is commonplace, and infections can rapidly enter from other countries. To ensure that potential risks are identified, Canadian Blood Services needs to be connected with the latest infectious disease information at all times. Canadian Blood Services’ medical and scientific staff participate in public health and infectious disease professional organizations and monitor web sites and journals where new information is posted. When appropriate the Alliance of Blood Operators (ABO) Risk Based Decision Making Framework can be used to facilitate policy decision making. This ensures that relevant assessments including infectious risk to recipients, operational impact of strategies, stakeholder input and health economics are considered. A range of infectious agents that could emerge as a threat within Canada are being monitored.
Coronavirus disease 2019 (COVID-19)
SARS-CoV-2 is a novel coronavirus first identified in Wuhan, Hubei province of China in late 2019. It is responsible for a severe respiratory illness known as the 2019 coronavirus disease (COVID-19). Some people become extremely ill and can die from complications, while others experience mild symptoms and may not be aware of their infection. On March 11th, 2020 the World Health Organization declared COVID-19 to be a pandemic. Since then close to one million Canadians have received a COVID-19 diagnosis and 22,000 people have died. SARS- CoV-2 is not transmissible by blood transfusion, however it did impact on procedures for ensuring donor safety and blood collection. For details see Section 8.
SARS-CoV-2 (COVID-19) seroprevalence
Early in the pandemic with less than 500 confirmed cases across Canada (March 23rd, 2020), strict physical distancing measures were implemented in most provinces. As a result, the first wave of the epidemic peaked by the end of April and plateaued in July and August. A resurgence of infections began in late September 2020 and continues to grow across Canada. These statistics do not convey the true infection rate because some infections will not cause illness, others may not be severe enough for people to seek testing, and testing may be disproportionately directed to outbreaks. Testing for SARS-CoV-2 antibodies is important to understand what proportion of the population have already been infected (the seroprevalence) and to monitor infection over the course of the pandemic. These data can also be used to improve mathematical models to predict the course of infection and inform public health policy. In partnership with the COVID-19 Immunity Task Force, Canadian Blood Services is testing residual blood for SARS-CoV-2 antibodies. To date 124,976 samples from across Canada have been tested for SARS-CoV-2 antibodies. These seroprevalence surveys revealed seroprevalence during the first wave was less than 1%, rates increased in wave 2 but remain relatively low. Figure 3 shows the changes over time.
Image
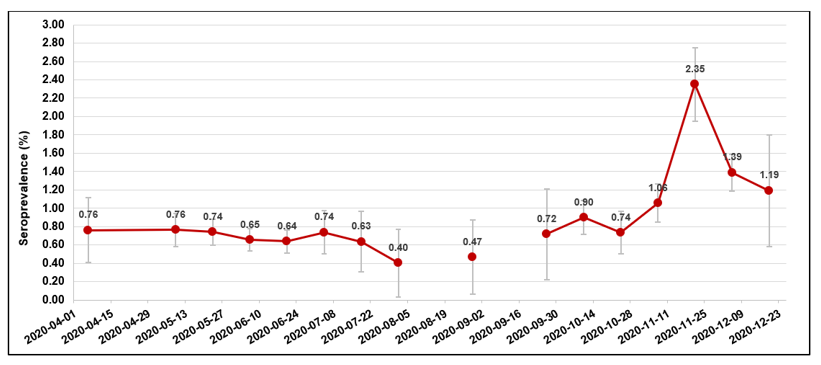
Figure 3: Seroprevalence estimates from April until December 2020.
Point estimates are indicated on the graph by approximately 2 week intervals, bars represent 95% Confidence Intervals. Testing was reduced over the late summer early fall, hence a break in the line.
Worldwide, blood services have leveraged their operational capacity to inform public health. SARS-CoV-2 seroprevalence remained low in Canada but there were significant variations by regions, racialized individuals and socioeconomic factors. Canadian Blood Services is committed to continuing to play a pivotal role in helping authorities evaluate public health policies, monitor disparities and track vaccine coverage in the future.
Babesiosis
Babesiosis comes from the bite of the black-legged tick (Ixodes scapularis) which can transmit the parasite B. microti. Usually it causes mild flu-like symptoms, and many people are not even aware that they have had it. However, it can also be transmitted by blood transfusion, and infection in blood recipients can result in severe illness or death. To date babesiosis cases in the general population have been reported mainly in the Northeastern and Upper Midwest parts of the United States where more than 1,500 cases per year are reported. Cumulatively more than 200 infections in the United States are believed to have been acquired from a transfusion. In Canada there has been one case of transfusion transmitted babesiosis in 1998 from a donor who had travelled to the Northeast US. In Canada the parasite is found in small numbers of ticks. A 2013 study at Canadian Blood Services and Héma-Québec tested 13,993 blood donations and none were positive. In 2013 one non-donor infected from a tick bite in Canada was reported. Ongoing public health surveillance of ticks suggests no increase in risk, but a donor study was carried out in 2018 involving more donors. One of 50,752 samples tested from southerly areas across Canada was positive by B. microti nucleic acid testing (NAT, donated in Manitoba and indicating an active infection) and of 14,758 samples tested for antibody to B. microti, 4 in Southwestern Ontario were positive (but negative by NAT, indicating likely resolved infection at some time in the past). In 2019 a donor developed illness after donating and was diagnosed with B. microti infection, likely infected in southern Manitoba. No recipients were infected from the donation. The estimated risk of a clinically relevant infection being transmitted from a blood transfusion in Canada is very low at 0.08 per year (0 – 0.38) per year, or about 1 in 12.5 years. The ABO Risk Based Decision Making Framework is being used to evaluate possible risk mitigation strategies.
Hepatitis E virus (HEV)
Hepatitis E is common in developing countries where it is spread through contaminated food and water. People can also be infected from eating undercooked pork. Similar to hepatitis A, healthy people often do not get very sick, generally clear the infection and never know they had it. However, blood recipients could become very ill. A 2013 study at Canadian Blood Services and Héma-Québec showed that 5.1% of donations were positive for antibody (indicating a previous infection with Hepatitis E) but none were positive for the virus. In 2015 a larger study (over 50,000 donations) with a more sensitive test identified 1 in 4,615 HEV positive donations. However, most were later stage infections with low concentrations of virus thus less likely to be infectious. The risk is lower than in some countries in Europe that have testing in place. The ABO Risk Based Decision Making Framework was used to consider strategies to address risk. The decision was to enhance physician awareness of HEV and enhance adverse event and donor surveillance.
Travel related infections
Donors who travel may return with infections that could be transmitted by blood (see Figure 4). Most are only a risk for a period of time after returning until they are eliminated from the donor’s bloodstream. Malaria risk is present in parts of the Caribbean, Mexico, Central and South America, Asia and Africa. Donors are deferred after travel to risk areas for 3 months, enough time to develop symptoms. Former residents of endemic areas are deferred for 3 years because there is a chance they may be infected longer without symptoms. Other tropical mosquito-borne infections such as dengue virus have long been present in sunny destinations frequented by Canadians, but in recent years there have been outbreaks of others such as Chikungunya virus and Zika virus not previously seen in the Caribbean, Mexico, Central and South America. Risk to the blood supply was determined to be very low based on quantitative risk assessment. However, to address future travel risks as of 2016 Canadian Blood Services defers all donors who have travelled anywhere outside of Canada, the USA or continental Europe for 3 weeks after travel. COVID-19 is circulating in Canada, but travel-related infections are also of concern, especially new variants that may be rare in Canada, hence a 2 week deferral for all travel outside of Canada that was not covered in the Zika risk deferral was implemented. This includes travel to the continental US and Europe.
Residency or cumulative travel considered a risk for variant-Creutzfeldt Jakob disease (vCJD) result in permanent deferral. vCJD is acquired from eating infected meat (Bovine Spongiform Encephalitis, or BSE, known as “Mad Cow Disease”) in the UK, France and other European countries during the years of the BSE epidemic in cattle. Donors are deferred for time spent in those countries while infected meat may have been available. Infectious risks in other countries are closely monitored to decide if further action is needed.
Image
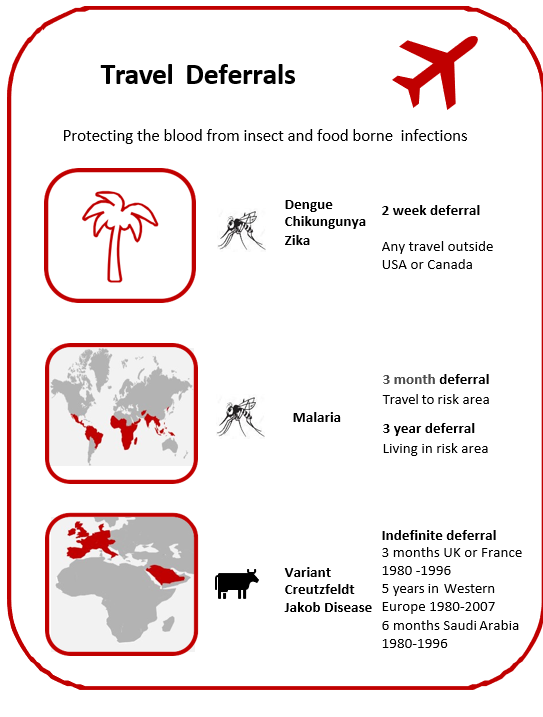
Figure 4: Key travel deferrals in place to reduce risk of transmissible infections
4. Bacteria
Bacteria in blood products usually come from the skin of donors during their blood donation, although occasionally they may come from the donor’s bloodstream. The number of bacteria is usually very low, but because platelet products are stored at room temperature, bacteria can multiply to reach high concentrations and then pose a serious risk to the recipient. Canadian Blood Services tests all apheresis and pooled platelet products for bacteria using the BACT/ALERT System in which a sample from the product is inoculated into an aerobic (presence of oxygen) culture bottle and an anaerobic (absence of oxygen) culture bottle and monitored for growth for 7 days. If any bacterial growth is detected in the culture bottles, the product is not issued if it is still in inventory at Canadian Blood Services. If it has been sent to a hospital, it is recalled and returned to Canadian Blood Services from the hospital blood bank (i.e., has not been transfused or discarded). In 2020, 105,720 platelet products (16,977 apheresis and 88,743 pooled products) were tested, of which 97 apheresis and 369 pooled products had initial positive results for bacterial growth in the culture bottles. From these, 6 and 118 cultures were confirmed as true bacterial contaminations, for apheresis and pooled products, respectively. In addition, 12 apheresis and 39 pooled products with initial positive results were not confirmed as they were issued and/or transfused. This represents 175 products in total (16.6 per 10,000) with a chance of bacterial contamination with current testing, including both true positives and suspected positives.
5. Donor eligibility criterion for male to male sex
In the 1980’s men who had sex with another man even once since 1977 were not eligible to donate blood to reduce the risk of HIV transmission. With much improved donor testing and surveillance for emerging pathogens the deferral period has been gradually reduced, moving to 5 years in 2013, to 1 year in 2016 and to 3 months in 2019. HIV rates did not increase following any of these changes (see Figure 5). Anonymous donor compliance surveys showed that shortening the deferral period allowed more MSM to donate blood and donor compliance was not adversely affected (see Figure 5). With these data the risk associated with reducing the deferral to 3 months was estimated to be 1 in 34.2 million donations (1 in 225,534 million, 8.7 million). Another compliance survey began in late 2020 to assess the impact of the 3-month deferral. Many countries have switched from lifetime to shorter time deferrals, mostly 3 months to 1 year. For example, England and recently the US have a 3 month deferral, and France and the Netherlands have 4 month deferrals.
Canadian Blood Services is committed to ongoing revision of this policy, ideally to find a way to more finely define donor sexual risk rather than deferring all sexually active MSM. In January of 2017 Canadian Blood Services and Héma-Québec hosted a meeting which included Canadian researchers in gay men’s health, regulatory staff (Health Canada and the USA Food and Drug Administration), stakeholders and international experts. The attendees brainstormed to identify the key areas of research needed to assess the safety of potential changes to the deferral. Canadian Blood Services and Héma-Québec then launched a competitive grant program to allocate funding provided by Health Canada to Canadian researchers. To date, 15 research projects are being funded in this grant program. In 2020 a second competitive grant program with funding provided by Health Canada focused on research related to plasma donation for MSM and 4 research projects were funded. For more information see: https://blood.ca/en/research/our-funded-research-projects?combine=msm
A meeting of grant-holders, regulatory staff (Health Canada and the USA Food and Drug Administration), stakeholders and international experts was convened in November 2019 at which research results were presented. For more information see https://www.blood.ca/en/blood/am-i-eligible/men-who-have-sex-men/knowledge-synthesis-interim-report. In December 2020 the grant-holders met again to share results.
Image
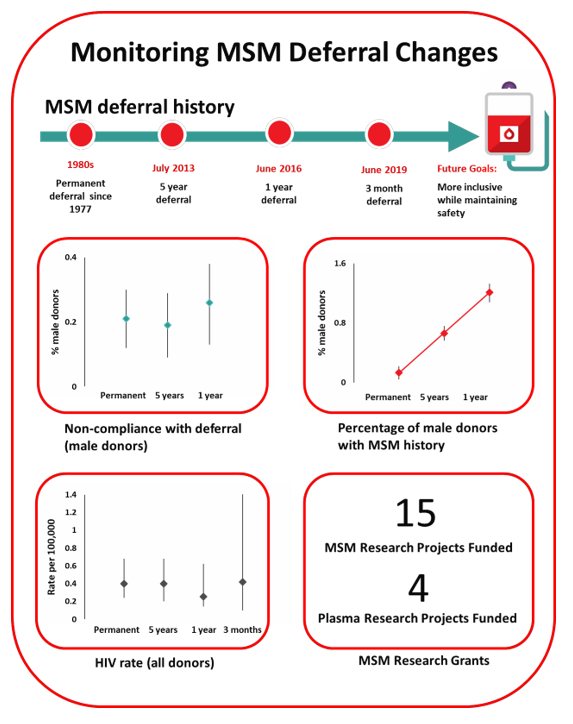
Figure 5: Increased eligible MSM donors but no change in non-compliance with the deferral or HIV rates as the durations of deferral periods were decreased.
6. Lookback/traceback
All cases of potential transfusion transmission of infections are investigated. The Lookback / Traceback Program is notified when a donor tests positive for a transmissible infection, or if the donor reports a transfusion transmissible infection after donating (even if it is not one that would normally be tested for). A Lookback investigation is initiated when previous or historical donations are identified, and hospitals are asked to contact the recipients of these donations to arrange testing. A traceback is initiated when a recipient is found to have a transmissible infection and transfusion was confirmed and it is queried as to whether their infection could have been from their blood transfusion. Hospitals provide a list of all blood products that the recipient received, and Canadian Blood Services attempts to contact the donors of these products to arrange testing unless current test results are available.
In 2020, there were 25 lookback cases that required investigation - 19 HCV, 3 HBV, 2 HTLV and 1 WNV. Ten of these were from donors who had a transmissible infection positive donation and 15 were from external testing or public health notification. Of these, 5 were cases closed (all recipients that could be contacted were tested). The remaining 20 cases were still open. There were 10 open cases from previous years that were closed in 2020. No closed cases were associated with transfusion transmission. There were 30 traceback cases that required investigation received from external sources in 2020 (2 HIV, 25 HCV, 3 HBV). Of these, 7 were closed (all donors that could be contacted were tested), and 23 remain open. There were also 13 cases from previous years closed. There were no closed cases associated with transfusion transmission.
7. Blood stem cells
Blood stem cells can multiply to renew themselves; the new cells develop into blood cells such as red cells, white cells and platelets. In adults, they are found mainly in the marrow of large bones, with a few cells in the bloodstream. The cord blood of newborn babies, taken from the umbilical cord and placenta after the delivery of a healthy baby, is also very rich in stem cells. Blood stem cells can therefore be obtained from the bone marrow, from circulating blood (called peripheral blood stem cells) or from the umbilical cord (cord blood) after a baby is born. Blood stem cells are very important in treating various types of diseases such as leukemia, lymphoma and multiple myeloma. Canadian Blood Services has a coordinated national stem cell program which includes adult registrants and banked cord blood units. Infectious disease testing for all stem cell products includes the same markers tested for whole blood donations.
Canadian Blood Services’ stem cell registry
Canadian Blood Services Stem Cell Registry is a registry of Canadians who have volunteered to donate either bone marrow or peripheral blood stem cells should a recipient need it at some time in the future. Potential registrants complete a questionnaire which includes risk factors for transmissible infections and are tested for their Human Leukocyte Antigen (HLA) profile. In 2020 there were about 457,000 registrants in the registry. In total, 156 registrants were identified as potential matches for recipients and had additional testing. This number is lower than previous years. This reduction was primarily caused by the COVID-19 pandemic and fewer registrants being selected for international patients due to travel restrictions affecting the transportation of stem cell donations. All tested registrants had negative results for all infectious disease markers.
Canadian Blood Services’ cord blood bank
Canadian Blood Services’ Cord Blood Bank collected cord blood at four sites in Canada in 2020 (Ottawa, Brampton, Edmonton, and Vancouver). Participating mothers at these hospitals who volunteer to donate their baby’s cord blood complete a questionnaire about medical conditions that could be passed on to a recipient, as well as risk factors for transmissible infections. If the donation is suitable for transplantation (i.e., has enough stem cells) with negative results for all infections, the cells are frozen and stored until a recipient needs them. In 2020, there were 283 blood samples from mothers tested and none were positive for any infections tested. This number is again lower than in previous years. This reduction is also due to the pandemic and having to suspend collections at all four sites during the first half of the year.
8. Donor safety
Donor reactions
Canadian Blood Services takes many precautions to make sure that giving blood is safe for donors. These include a health screening questionnaire and a hemoglobin fingerstick screen, as well as providing refreshments and monitoring the donor after donating. Most donors do not have any problems during or after their donation, but it is important to keep track of any incidents that happen so that donor care can be improved. Definitions of reactions are shown in Table 4.
Table 4: Reaction and definitions
| Reaction | Definition |
|---|---|
| Vasovagal
Moderate Severe |
Donor loses consciousness (faint reactions)
Unconscious less than 60 seconds and no complications Unconscious more than 60 seconds or complications |
| Major Cardiovascular Event | Chest pain or heart attack within 24 hours of blood donation, may or may not be related to donation |
| Re-bleed | The phlebotomy site starts to bleed after donation |
| Nerve Irritation | Needle irritation or injury of a nerve during phlebotomy. Usually described as sharpshooting pain, arm tingling or numbness |
| Inflammation/Infection | Redness or infection at the needle site, usually seen several days after donating |
| Local Allergic Reaction | Rash from skin cleaning solution or dressing, with raised vesicles on the skin |
| Arm Pain | Usually due to blood pressure cuff, tourniquet or arm position |
| Bruise/Hematoma | Temporary dark colour of the skin due to blood leakage from blood vessel at time of phlebotomy |
| Arterial Puncture | Needle inserted in an artery instead of a vein |
Reaction rates per 10,000 whole blood donations in 2020 are shown in Figure 6 with those in 2019 for comparison. Moderate vasovagal reactions were lower (p= 0.03) and severe reactions trended downwards, but the change was not statistically significant (p >0.05). People more likely to experience a reaction are first-time donors, young donors (17-25 years old) and female donors. The reaction reporting system is oriented towards capturing moderate and severe reactions. Most reactions are mild, such as feeling faint or bruising at the needle site, but these are only recorded if mentioned by the donor at some point after donation. A further breakdown of fainting reactions (both moderate and severe) in whole blood donors by sex and donation history is provided in Table 5. Due to small numbers in each group these are not significantly different from those reported in 2019 (p>0.05), except for female repeat donors with injuries where an increase in the number is observed in 2020 (p<0.01).
Cardiovascular events are very rare. It is difficult to know if cardiovascular events that happen shortly after donation are in any way related to donation, or simply happened by chance in the 24 hours after donation.
Image
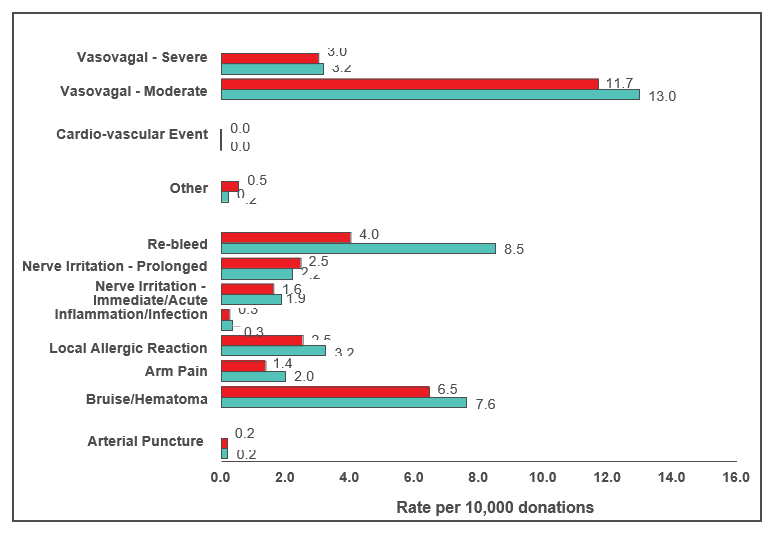
Figure 6: Reaction rates per 10,000 whole blood donations in 2020 (red) and 2019 (green)
Table 5: 2020 Fainting (vasovagal) reactions (per 10,000 collections)
| Donation Status | Moderate & Severe (all)* | Associated with injury*‡ | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| First Time | 44.8 | 67.7 | 1.0 | 3.7 |
| Repeat | 5.0 | 17.1 | 0.3 | 1.8 |
|
*all comparisons are statistically significant among moderate & severe reactions combined (p<0.05). For reactions associated with injury all were significant except first-time vs repeat males. ‡Injuries were generally not severe such as bruises and cuts from falling. |
||||
To reduce the risk of COVID-19 infection collection sites provided post-donation refreshments as always but asked donors to have them outside of the clinic. Collection sites stopped providing salty snacks and water before donating, although donors were encouraged to have their own before coming to the clinic. Pre-donation water and salty snacks were put in place in 2019 to reduce vasovagal (faint) reactions. Donor instructions to carry out muscle tension exercises while donating continued to be provided. These can also reduce the risk of a vasovagal reaction. Collectively the pre-donation water and salty snacks and muscle tension exercises are called Donor Wellness activities. Figure 7 shows the reaction rates before putting in place the Donor Wellness activities, while they were in place and after stopping the pre- donation water and salty snacks. There was a downward trend in vasovagal reactions for all groups, but only statistically significant male repeat donors (p<0.01) and marginally significant for female repeat donors (p=0.05) There were no changes after Donor Wellness activities were modified to reduce COVID-19 risk (p>0.05).
Image
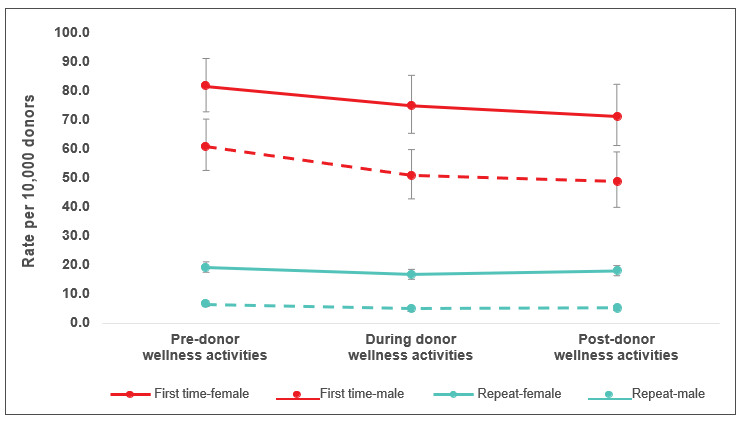
Figure 7: Moderate and severe vasovagal reactions pre-donor wellness activities (April - December 2018), during donor wellness activities (April - December 2019), and post-ceasing donor wellness activities due to COVID-19 safety measures (April - December 2020).
COVID-19 and donor safety
There is currently no evidence that SARS-CoV-2 is blood transmissible. However, there are concerns about (1) infectious risks to donors, volunteers and staff at donation sites and (2) risks to the adequacy of the blood supply. Figure 8 summarizes some of the operational changes that were implemented before and after donors entered collection sites. As shown in Figure 9 a little over 1% of donors were turned away at the pre-screen wellness check point. In March a -2- week deferral for travel outside Canada was put in place (previously only travel outside Canada, the US and Europe in the last 3 weeks was deferrable). In addition, donors were deferred for 2 weeks after recovery from COVID-19 and for 2 weeks if they had been in contact with someone who had COVID-19. Later donors who had been hospitalized for COVID-19 were deferred for 3 weeks after recovery. The number of people who entered the clinic and were then deferred for COVID-19 or COVID-19 risks was also very low (0.2%). Canadian Blood Services was able to maintain the adequacy of the blood supply, which remained above target from January- December 2020 (Figure 10). In certain periods of the year, lower demand was seen since elective surgeries were cancelled across Canada to ensure there was enough room in hospitals for COVID-19 patients.
As shown in Figure 11 there were somewhat fewer male donors during the COVID-19 pandemic period compared with the same time frame in the previous two years. The first-time donor rate continued to decrease similar to the previous two years, and the proportions of donations from young donors (17 – 29) decreased and from donors 50 or over increased, both continuing trends seen pre-COVID-19.
Image
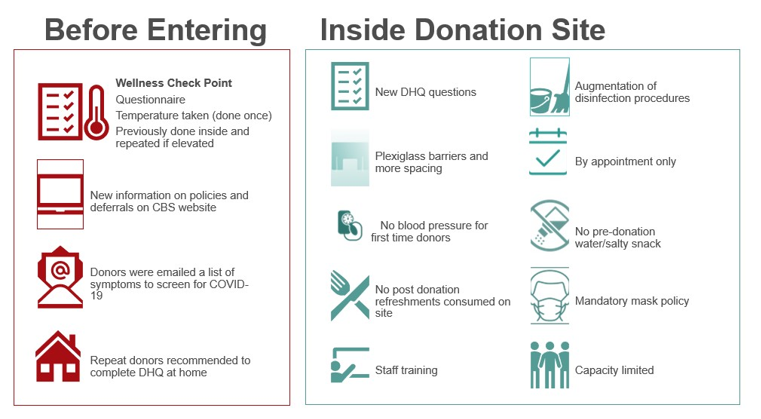
Figure 8: Key changes in the donation clinic to protect donors and staff during the COVID-19 pandemic
Image
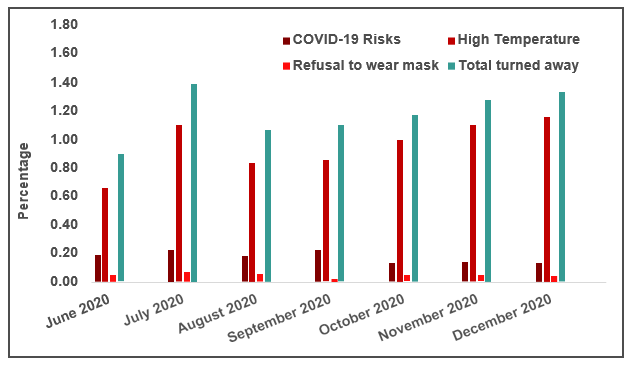
Figure 9: Frequency of donors turned away at the pre-screen
Image
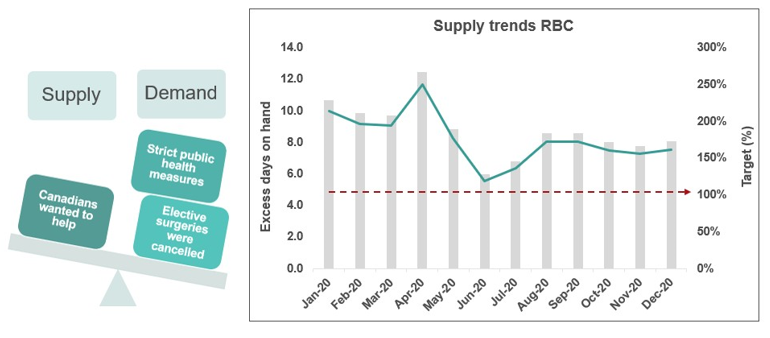
Figure 10: Factors affecting supply and demand. The target for the blood supply has consistently been to maintain five days on hand in inventory at Canadian Blood Services (red dashed line).
Image
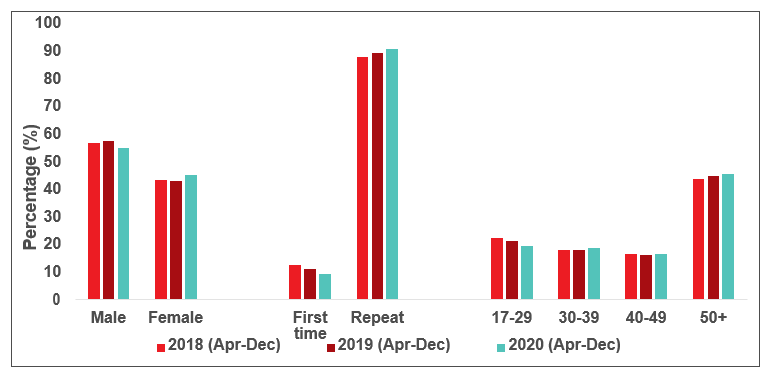
Figure 11: Donations by demographic variables pre-COVID -19 (2018 and 2019) and during the COVID-19 pandemic
Donor hemoglobin and iron
The most common reason for a donor deferral at the collection site is a failed hemoglobin fingerstick screen. Low hemoglobin is often related to low iron stores. Iron is needed to make hemoglobin which carries oxygen in red blood cells. Studies at Canadian Blood Services showed that iron stores are often lower in females and are further reduced by frequent donation in both females and males. Males with borderline hemoglobin are also more likely to have lower iron stores. To reduce the chance of developing iron deficiency, the minimum wait time between whole blood donations for females was increased from 56 days to 84 days in 2017. This longer interdonation period allows females more time to build back their iron stores and return to their baseline hemoglobin levels. To reduce the chance of blood shortages if fewer people donated during the pandemic, the minimum hemoglobin was dropped from July to October to 120 g/L for females and 125 g/L for males. The deferrals decreased from 7% to 3.2% (p<0.01) for females and from 1.5% to 0.8% (p<0.01) for males during that period.
Information about iron and the safety of blood donation can be found at www.blood.ca as well as in the ‘What you must know to give blood’ pamphlet provided to all donors prior to every donation.
9. Diagnostic services
Image
The Diagnostics Services Laboratories provide patient testing, mainly for pregnant women (Perinatal Laboratories) and patients receiving blood transfusions (Crossmatch/Reference Laboratories). Some Canadian Blood Services Diagnostic Services Laboratories provide all of these services
| Maternal | 97.77% |
| Paternal | 0.74% |
| Cord | 1.49% |
| 165,756 samples tested |
Perinatal laboratories
The Perinatal Laboratories provide testing of pregnant women for blood group and antibodies to red blood cells. Some antibodies can cause hemolytic disease of the fetus/newborn. The goal is to (1) identify Rh negative pregnant women and recommend treatment to prevent developing anti-D antibodies, and (2) identify pregnant women with risky antibodies to monitor their pregnancy and treat as needed. Testing of fathers, newborns and fetuses is also sometimes done. In 2020 1,160 women had red blood cell antibodies; the most common ones that could put their baby at risk are shown in Figure 12.
Image
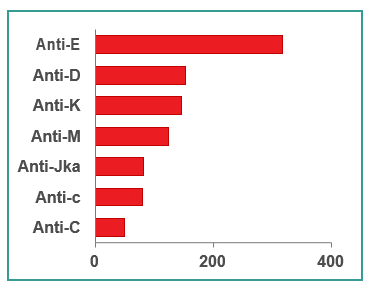
Figure 12: Number of clinically significant perinatal antibodies, 2020
Crossmatch/reference laboratories
The reference laboratories provide testing of patients for blood groups which must match the donor blood to be transfused. They also carry out antibody investigations for patients who may have unusual red blood cell antibodies and need special matching of blood for transfusion. Figure 13 shows the frequency of different antibodies in pre-transfusion patients (1,430 patients). Patients who have rare antibodies/antigens may be difficult to match for transfusion. The National Platelet Immunohematology Platelet Reference Lab in Winnipeg, Manitoba assists health care providers manage thrombocytopenic patients by HLA and Human Platelet Antigen (HPA) typing and investigation for HLA and HPA. HLA and HPA typed platelets are available for transfusion support of these patients.
For more detail see https://blood.ca/en/hospital-services/laboratory-services/surveys
Image
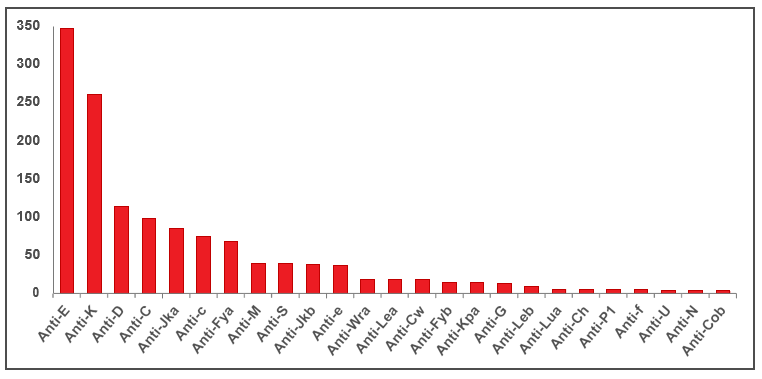
Figure 13: Number of reference antibodies, 2020
References
Donor Screening
Goldman M, Shih A W-Y, O’Brien SF, Devine D. Donor deferral policies for men who have sex with men: past, present and future. Vox Sang 2018; 113:95-103.
O’Brien SF, Osmond L, Fan W, Yi QL, Goldman M. Compliance with time based deferrals for men who have sex with men. Transfusion 2019; 59:916-920.
O’Brien SF, Goldman M, Robillard P, Osmond L, Myhal G, Roy E. Donor screening question alternatives to men who have sex with men time deferral: Potential impact on donor deferral and discomfort. Transfusion 2021;61:94-101.
Saeed S, Goldman M, Uzicanin S, O’Brien SF. Evaluation of a Pre-exposure Prophylaxis (PrEP)/ Post Exposure Prophylaxis (PEP) Deferral Policy among Blood Donors Transfusion 2021;doi:10.1111/trf.16349
Goldman M, Germain M, Gregoire Y, Vassallo RR, Kamel H, Bravo M, O’Brien SF. Safety of blood donation by individuals over age 70 and their contribution to the blood supply in five developed countries: a BEST Collaborative group study. Transfusion 2019; 59:1267-1272.
Residual Risk
O’Brien SF, Yi Q-L, Fan W, Scalia V, Goldman M, Fearon MA. Residual risk of HIV, HCV and HVB in Canada. Transfus and Apher Sci 2017; 56:389-391.
O’Brien SF, Gregoire Y, Pillonel J, Steele WR, Custer B, Davison K, Germain M, Lewin A, Seed CR. HIV residual risk in Canada under a three-month deferral for men who have sex with men. Vox Sang 2020;115:133-139.
Babesia microti
O’Brien SF, Delage G, Scalia V, Lindsay R, Bernier F, Dubuc S, Germain M, Pilot G, Yi QL, Fearon MA. Seroprevalence of Babesia microti infection in Canadian blood donors.
Transfusion 2016;56:237-243.
Tonnetti L, O’Brien SF, Gregoire Y, Proctor MC, Drews SJ, Delage G. Prevalence of Babesia in Canadian blood donors: June-October 2018. Transfusion 2019;59:3171-3176.
Hepatitis E
Fearon MA, O’Brien SF, Delage G, Scalia V, Bernier F, Bigham M, Weger S, Prabhu S, Andonov A. Hepatitis E in Canadian blood donors. Transfusion 2017;57:1420-1425.
Delage G, Fearon M, Gregoire Y, Hogema BM, Custer B, Scalia V, Hawes G, Bernier F, Nguyen ML, Stramer S. Hepatitis E virus infection in blood donors and risks to patients in the United States and Canada. Trans Med Rev 2019;33:139-145.
Bacteria
Ramirez-Arcos S, DiFranco C, McIntyre T, Goldman M. Residual risk of bacterial contamination of platelets: six years of experience with sterility testing. Transfusion 2017;57:2174-2181.
Ramirez-Arcos S, Evand S, McIntyre T, Pang C, Yi QL, DiFranco C, Goldman M. Extension of platelet shelf life with an improved bacterial testing algorithm. Transfusion 2020;60:2918-2928.
Malaria
O’Brien SF, Ward S, Gallian P, Fabra C, Pillonel J, Davison K, Seed CR, Delage G, Steele WR, Leiby DA Malaria blood safety policy in five non-endemic countries: a retrospective comparison through the lens of the ABO risk-based decision-making framework. Blood Transfus 2019;17:94-102.
HTLV
O’Brien SF, Yi QL, Goldman M, Gregoire Y, Delage G. Human T-cell lymphotropic virus: A simulation model to estimate residual risk with universal leukoreduction and testing strategies in Canada. Vox Sang 2018;113:750-759
Zika Virus
Germain M, Delage G, O’Brien SF, Grégoire Y, Fearon M, Devine D. Mitigation of the threat posed to transfusion by donors traveling to Zika-affected areas: a Canadian risk-based approach. Transfusion 2017;57:2463-2468.
Murphy MS, Shehata N, Colas JA, Chassé M, Fergusson DA, O’Brien SF, Goldman M, Tinmouth A, Forster AJ, Wilson K. Risk of exposure to blood products during pregnancy: guidance for Zika and other donor deferral policies. Transfusion 2017;57:811-815.
Iron Deficiency
O’Brien SF, Goldman M. Understanding iron depletion and overload in blood donors. ISBT Science Series 2017;12:11-18.
Goldman M, Uzicanin S, Osmond L, Scalia V, O’Brien SF. A large national study of ferritin testing in Canadian blood donors. Transfusion 2017;57:564-570.
Goldman M, Yi QL, Steed T, O’Brien SF. Changes in minimum hemoglobin and interdonation interval: impact on donor hemoglobin and donation frequency. Transfusion 2019;59:1734-1741.
Appendix I: Implementation dates of testing
| Marker | Implementation Date* | ||
|---|---|---|---|
| 1 | Syphilis | 1949 | |
| 2 |
HBV (Hepatitis B Virus) |
||
|
|
HBsAg |
1972 |
|
|
|
Anti-HBc |
2005 |
|
|
|
HBV NAT |
2011 | |
| 3 |
HIV (Human Immunodeficiency Virus) |
||
| Anti-HIV-1 EIA (enzyme-linked immunosorbent assay) | 1985 | ||
|
Anti-HIV-1/2 EIA |
1992 | ||
| HIV-1 p24 antigen | 1996 (discontinued in 2003) | ||
| HIV-1 NAT | 2001 | ||
| Anti-HIV-1/2 (including HIV-1 subtype O) EIA | 2003 | ||
| 4 |
HTLV (Human T-Lymphotropic Virus) |
||
| Anti-HTLV-I | 1990 | ||
| Anti-HTLV-I/II | 1998 | ||
| 5 |
HCV (Hepatitis C Virus) |
||
| Anti-HCV EIA/ELISA | 1990 | ||
| HCV NAT | 1999 | ||
| 6 |
WNV (West Nile Virus) |
||
| WNV NAT | 2003 | ||
| 7 | Chagas’ disease (Trypanosoma cruzi) selective testing | 2010 | |
| 8 | Bacteria | ||
| BacT Alert | 2004 | ||
| BacT Alert modified for 7 day platelets | 2017 | ||
|
*These are the dates that testing for the marker began. Tests have been upgraded as new versions of the test became available. |
|||
Appendix II: Rate of HIV, HCV, HBV, HTLV and syphilis in first-time and repeat donations
Image
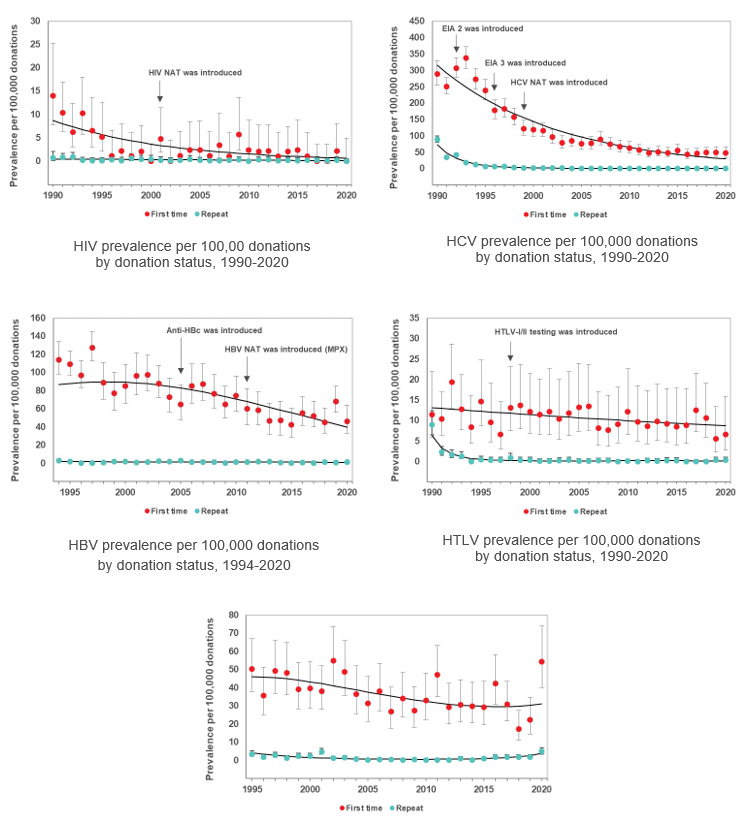
Figure 14: Rate of HIV, HCV, HBV, HTLV and syphilis in first-time and repeat donations
(Note that these graphs have different scales on the y-axis)